HL only: Fatigue and recovery
· Additional higher level: 9 hours — this whole subtopic is HL-only.
· Fatigue = reduced ability to maintain the required force, power, speed, skill execution or exercise intensity.
· Fatigue can originate at different points in the motor pathway and energy pathway.
· Fatigue is usually multifactorial: several mechanisms may combine rather than one single cause.
· Exam focus: explain how fuel depletion, ion imbalance, metabolite accumulation, dehydration, hyperthermia and poor recovery reduce performance.
Fatigue: where it can originate
· Central fatigue = fatigue linked to the central nervous system, reducing neural drive, motivation or voluntary activation of muscles.
· Peripheral fatigue = fatigue within or near the working muscles, reducing contraction force or speed.
· Fatigue can affect the pathway from brain/spinal cord → motor neuron → neuromuscular junction → muscle fibre → ATP supply → cross-bridge cycling.
· In exams, link the cause to the performance outcome: less ATP availability, reduced excitation–contraction coupling, reduced force production, slower movement, or increased perceived exertion.
Fuel availability and fatigue
· Insufficient fuel availability contributes to fatigue because muscles need fuel to resynthesise ATP.
· Phosphocreatine (PCr) depletion reduces rapid ATP resynthesis during short, high-intensity exercise.
· Muscle glycogen depletion limits carbohydrate availability in the working muscle, especially during prolonged or repeated high-intensity exercise.
· Liver glycogen depletion reduces the body’s ability to maintain blood glucose, increasing fatigue risk during longer exercise.
· Low fuel availability can increase perceived exertion, reduce power output, impair skill execution, and speed up the onset of exhaustion.
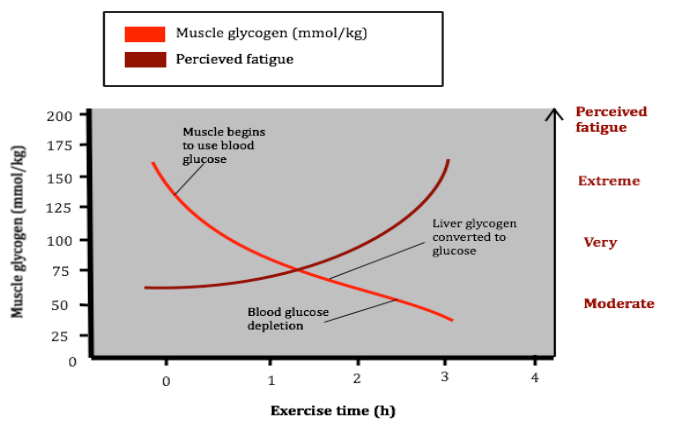
This graph links falling muscle glycogen stores with rising perceived fatigue during endurance exercise. It helps students connect fuel depletion to reduced ability to maintain performance intensity. Source
Ion imbalance, acidosis and inorganic phosphate
· Changes in sodium ions (Na⁺) and potassium ions (K⁺) can disrupt nerve impulse transmission and muscle fibre excitability.
· During intense exercise, K⁺ can accumulate outside muscle fibres, making it harder to maintain effective action potentials.
· Acidosis = increased acidity due to accumulation of hydrogen ions (H⁺); it can interfere with enzyme activity and contraction processes.
· Inorganic phosphate (Pi) accumulates when ATP and PCr are broken down; high Pi can impair cross-bridge function and calcium handling.
· Key exam phrase: metabolite accumulation reduces excitation–contraction coupling and force production.
Dehydration, hyperthermia and performance impairment
· Dehydration reduces body water and can reduce plasma volume, increasing cardiovascular strain.
· Hyperthermia = excessive rise in body temperature; it increases physiological stress and can reduce exercise tolerance.
· Together, dehydration and hyperthermia can impair the cardiovascular system by making it harder to maintain blood flow to both working muscles and skin for cooling.
· Likely effects: increased heart rate, reduced stroke volume, reduced thermoregulation, higher perceived exertion, and earlier fatigue.
· In exam answers, link hot/humid conditions to sweat loss → dehydration → cardiovascular strain → performance impairment.
Recovery: what counts as recovery?
· Recovery from exercise means returning toward a state where the athlete can perform effectively again.
· Physiological indicators: reduced blood lactate concentration, restored hydration, restored fuel stores, normalised heart rate or reduced thermal strain.
· Symptomatic indicators: reduced muscle soreness, reduced stiffness, improved movement quality.
· Psychological indicators: improved preparedness, motivation and confidence for the next session or competition.
· Strong exam answers classify recovery signs as physiological, symptomatic or psychological.
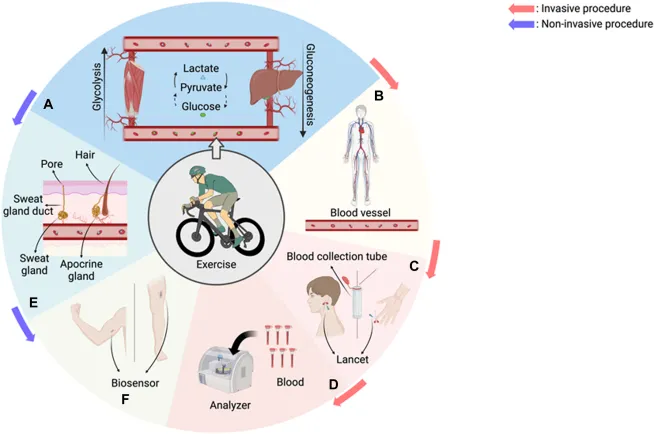
This figure shows how lactate is produced during exercise and how it can be monitored. It supports the syllabus point that reduced blood lactate concentration is a physiological indicator of recovery. Source
Nutritional strategies for recovery
· Water: restores fluid balance, supports thermoregulation and helps reduce cardiovascular strain after exercise.
· Carbohydrates: replenish muscle glycogen and liver glycogen, especially after endurance or repeated high-intensity work.
· Protein: supports muscle repair, adaptation and tissue synthesis after damaging or resistance-based exercise.
· Macronutrient timing and amount depend on the activity goal, training load and time before the next session.
· Creatine monohydrate: supports recovery of phosphocreatine stores and repeated high-intensity performance capacity.
· Polyphenol-rich foods may support recovery by helping manage exercise-induced oxidative stress and inflammation, but should be evaluated rather than assumed to be essential.
· Evaluation point: a strategy is only useful if it matches the athlete’s event demands, fatigue cause, recovery time available and individual tolerance.
Recovery techniques
· Myofascial release: aims to reduce muscle tightness or soreness and improve perceived readiness; evidence and effect size may vary.
· Compression garments: may support venous return or reduce perceived soreness, but effects depend on duration, fit and sport context.
· Thermotherapy = use of heat or cold-based methods to influence recovery.
· Cold-based methods may reduce soreness and thermal strain, but may not always be ideal if the goal is maximum training adaptation.
· Heat-based methods may increase blood flow and relaxation, but should be used carefully after heat stress or dehydration.
· Exam evaluation: avoid saying a technique “always works”; discuss benefits, limitations and context.
Sleep and recovery
· Sleep quality affects both recovery and performance.
· Sleep supports muscle repair, hormonal regulation, immune function, learning, mood and psychological readiness.
· The amount of sleep required beyond general recommendations depends on training load.
· Heavy training, competition stress or travel may increase sleep need or reduce sleep quality.
· Travel across or within time zones can disrupt sleep timing and quality.
· Sleep-adjustment methods may include gradually shifting bedtime, managing light exposure, planning naps, reducing caffeine late in the day and keeping a consistent routine.
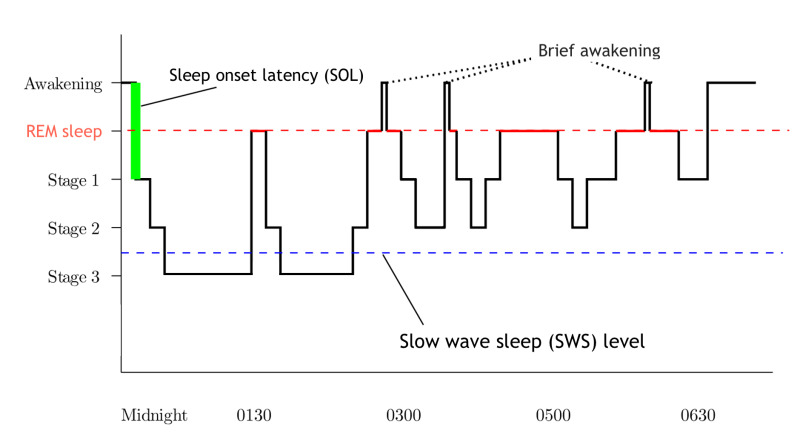
This hypnogram shows how sleep cycles through NREM and REM stages across the night. It helps students understand why sleep quality and timing matter for recovery, not just total hours in bed. Source
Exam application: matching fatigue cause to recovery strategy
· PCr depletion → allow rest between maximal efforts; consider creatine monohydrate for repeated high-intensity performance contexts.
· Glycogen depletion → prioritise carbohydrate intake after exercise, especially when sessions are close together.
· Dehydration or hyperthermia → prioritise water, cooling, shade and monitoring of heat stress symptoms.
· Muscle soreness → consider sleep, nutrition, myofascial release, compression garments or appropriate thermotherapy.
· Psychological fatigue or low readiness → prioritise sleep quality, reduced training load, recovery routines and motivational support.
Checklist: can you do this?
· Explain how central and peripheral fatigue differ.
· Link PCr depletion, glycogen depletion, ion changes, acidosis and inorganic phosphate to reduced performance.
· Explain how dehydration and hyperthermia impair the cardiovascular system during exercise.
· Classify recovery signs as physiological, symptomatic or psychological.
· Evaluate whether nutrition, sleep or recovery techniques are appropriate for a given athlete, sport and recovery time.