
OCR Specification focus:
‘Explain ultrafiltration, selective reabsorption and urine formation in the mammalian kidney.’
The mammalian kidney performs filtration and reabsorption to produce urine, maintaining blood composition and volume through precisely regulated processes ensuring homeostasis and the removal of metabolic wastes.
Kidney Function Overview
The kidney is the main organ responsible for removing nitrogenous wastes and regulating water, ion, and pH balance. Each kidney contains about a million nephrons, which are the functional units where filtration and reabsorption occur. These processes together ensure that essential substances are retained while wastes and excess water are excreted as urine.
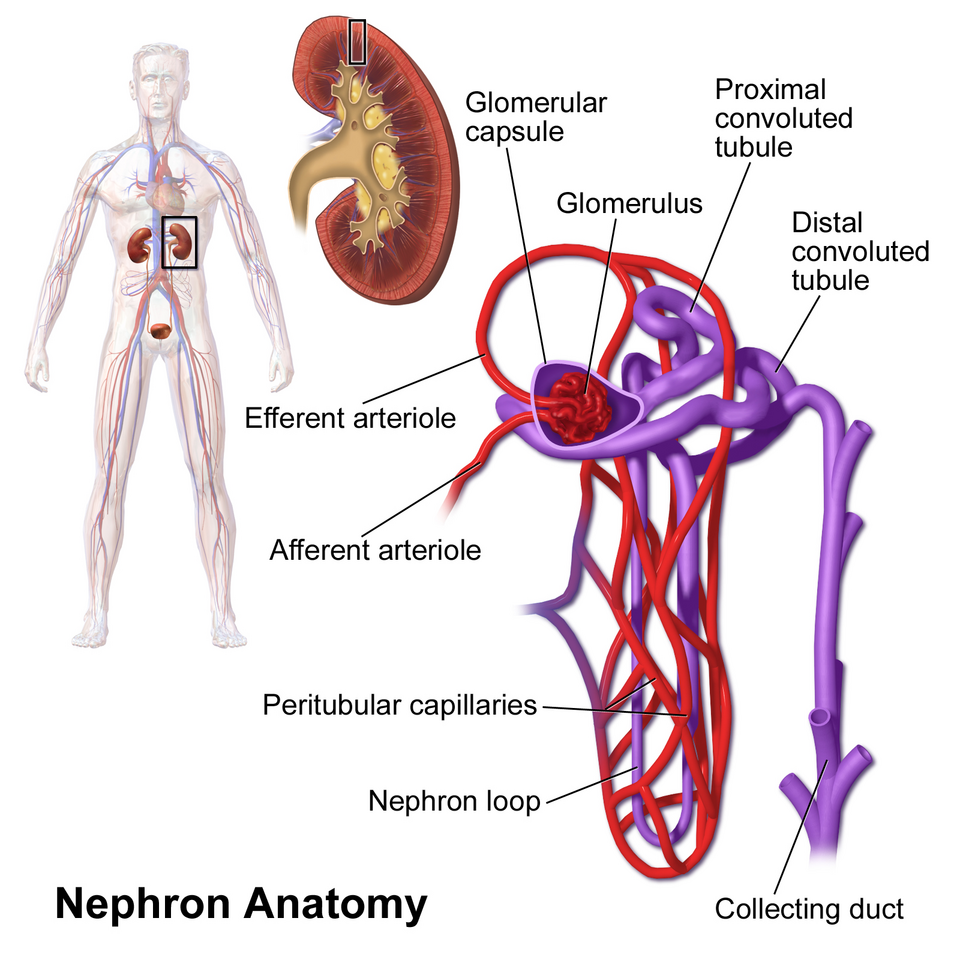
Labelled illustration of a nephron showing the renal corpuscle, PCT, loop of Henle, DCT, and collecting duct, plus arterioles and capillaries. Useful for orienting the sites of ultrafiltration and subsequent reabsorptive steps described in the text. Labels are concise and align with OCR terminology. Source.
Ultrafiltration in the Renal Corpuscle
The Structure of the Renal Corpuscle
Each nephron begins with a Bowman’s capsule surrounding a network of capillaries called the glomerulus. Blood enters through the afferent arteriole and exits via the efferent arteriole, which has a smaller diameter. This difference creates a high hydrostatic pressure within the glomerulus, driving filtration.
Ultrafiltration: The process by which small molecules such as water, glucose, urea, and ions are forced out of the blood into the Bowman’s capsule under high pressure.
Filtration Barriers
The filtration barrier between the blood and the Bowman’s space consists of three layers:
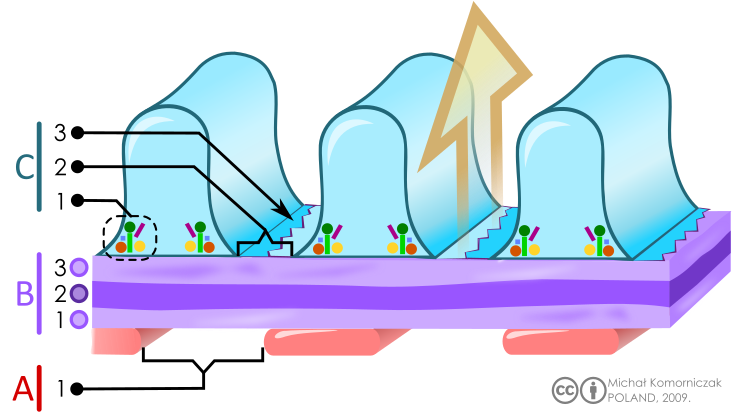
Schematic of the glomerular filtration barrier, labelling fenestrated endothelium, the glomerular basement membrane (lamina rara interna, lamina densa, lamina rara externa), and podocyte filtration slits. It illustrates how size and charge selectivity underlie ultrafiltration. The lamina sub-layers are shown for clarity and may exceed the granularity typically required in OCR summaries. Source.
Endothelium of glomerular capillaries: contains pores allowing passage of plasma components.
Basement membrane: acts as a selective barrier preventing large molecules, such as plasma proteins, from passing through.
Podocytes: specialised epithelial cells with filtration slits that further regulate what enters the glomerular filtrate.
Only molecules with a relative molecular mass below about 69,000 can pass through. Thus, glucose, amino acids, ions, urea, and water form part of the filtrate, while red blood cells and large proteins remain in the blood.
Formation of Glomerular Filtrate
Filtration occurs because of the balance between hydrostatic pressure in the glomerulus and osmotic and capsular pressures opposing it.
EQUATION
—-----------------------------------------------------------------
Net Filtration Pressure (NFP) = Glomerular Hydrostatic Pressure – (Blood Oncotic Pressure + Capsular Hydrostatic Pressure)
NFP = overall pressure driving filtration into the Bowman’s capsule.
—-----------------------------------------------------------------
The resulting glomerular filtrate has a composition similar to plasma but without proteins. This filtrate then moves into the proximal convoluted tubule (PCT) for selective reabsorption.
Selective Reabsorption in the Proximal Convoluted Tubule
Structure of the PCT
The PCT is adapted for efficient reabsorption with:
Cuboidal epithelial cells possessing numerous microvilli to increase surface area.
Mitochondria providing ATP for active transport processes.
Tight junctions preventing leakage of substances back into the filtrate.
Substances Reabsorbed
Approximately 85% of the filtrate is reabsorbed here. Key processes include:
Active transport of sodium ions (Na⁺) out of the tubular cells into the blood via the sodium–potassium pump.
Co-transport of glucose and amino acids with Na⁺ ions from the filtrate into tubular cells.
Water follows by osmosis due to the lowered water potential.
Chloride ions (Cl⁻) and urea are reabsorbed by diffusion.
Selective Reabsorption: The process by which useful substances such as glucose, amino acids, ions, and water are reabsorbed from the nephron back into the blood.
All glucose and amino acids are normally reabsorbed. If blood glucose exceeds the renal threshold, as in diabetes mellitus, some remains in the urine.
Reabsorption in the Loop of Henle
Role in Water Potential Regulation
The Loop of Henle creates a countercurrent multiplier system that concentrates the medulla, allowing water reabsorption later in the collecting duct.
Descending limb: permeable to water but not ions. Water leaves by osmosis into the increasingly salty medulla.
Ascending limb: impermeable to water; actively transports Na⁺ and Cl⁻ ions out into the medulla.
This establishes a water potential gradient so that water can be conserved efficiently.
Countercurrent Multiplier: A mechanism that uses energy to generate a concentration gradient, enabling water reabsorption and the production of concentrated urine.
Reabsorption in the Distal Convoluted Tubule and Collecting Duct
The Distal Convoluted Tubule (DCT) fine-tunes ion balance. Here:
Na⁺ and Cl⁻ ions may be reabsorbed in exchange for K⁺ ions, under the influence of aldosterone.
Ca²⁺ reabsorption may also occur under hormonal control.
In the collecting duct, water reabsorption is regulated by antidiuretic hormone (ADH), secreted from the posterior pituitary. ADH increases the permeability of the collecting duct walls by stimulating the insertion of aquaporins (water channels) into the membrane, allowing more water to be reabsorbed into the bloodstream.
Formation of Urine
After selective reabsorption and water adjustment:
The remaining filtrate consists mainly of urea, excess ions, and water.
This is the urine, which flows through the renal pelvis, ureter, and into the bladder for storage before excretion.
Typical composition of urine:
Water (around 95%)
Urea and other nitrogenous wastes
Excess ions (e.g. Na⁺, Cl⁻, K⁺, H⁺)
Creatinine and small quantities of uric acid
Healthy urine does not contain glucose, large proteins, or blood cells, as these are normally retained in the bloodstream.
Summary of Key Processes
Ultrafiltration occurs in the glomerulus, producing a protein-free filtrate.
Selective reabsorption in the PCT retrieves essential nutrients and water.
The Loop of Henle maintains the medullary gradient for water conservation.
Hormonal control in the DCT and collecting duct ensures appropriate final water content.
The final urine reflects homeostatic control of solute and water balance.
Practice Questions
Question 1 (2 marks)
Explain how the structure of the glomerulus and Bowman’s capsule allows ultrafiltration to occur.
Mark scheme:
High hydrostatic pressure in the glomerulus due to the narrower efferent arteriole compared with the afferent arteriole (1 mark).
The filtration barrier made up of fenestrated capillary endothelium, basement membrane, and podocytes allows small molecules (e.g. water, glucose, ions) to pass through but prevents large molecules and blood cells (1 mark).
Question 2 (5 marks)
Describe and explain how selective reabsorption of glucose and water occurs in the proximal convoluted tubule.
Mark scheme:
Glucose and amino acids are reabsorbed from the filtrate by co-transport with sodium ions (Na⁺) through specific carrier proteins in the PCT epithelial cells (1 mark).
Sodium–potassium pumps actively transport Na⁺ out of the epithelial cells into the blood, maintaining a concentration gradient that allows Na⁺ (and co-transported substances) to diffuse in from the filtrate (1 mark).
This process requires ATP from numerous mitochondria in the PCT cells (1 mark).
As solutes are reabsorbed, the water potential in the filtrate decreases, causing water to move by osmosis into the surrounding capillaries (1 mark).
Tight junctions between the epithelial cells prevent leakage, ensuring reabsorbed substances enter the bloodstream efficiently (1 mark).
FAQ
The basement membrane acts as the main filtration barrier. It consists of a fine mesh of collagen and glycoproteins that repel negatively charged molecules and prevent large proteins from passing through.
Its pores allow only small molecules, such as glucose, amino acids, ions, and water, to enter the filtrate.
Molecules larger than approximately 69 kDa are retained in the blood.
The negative charge of both the membrane and plasma proteins provides electrostatic repulsion, ensuring selective permeability.
The PCT reabsorbs about 85% of the filtrate because of its structural specialisations:
Microvilli provide a vast surface area for transport.
Mitochondria supply ATP for active transport processes.
Tight junctions ensure one-way movement of solutes into the blood.
These adaptations make the PCT highly efficient for reclaiming essential nutrients before the filtrate reaches the loop of Henle, where water balance becomes the priority.
Ultrafiltration depends on high glomerular hydrostatic pressure. If both arterioles had equal diameters, this pressure difference would disappear.
Reduced pressure would mean less filtrate is forced through the glomerular barrier.
Essential wastes such as urea might not be filtered effectively.
Blood would retain excess fluid, disrupting osmotic balance and leading to toxin accumulation.
Thus, the narrower efferent arteriole is vital for maintaining filtration pressure.
Plasma proteins are too large and often negatively charged, preventing them from passing through the filtration barrier.
The basement membrane’s pore size restricts macromolecules.
The negative charge on both proteins and the membrane causes electrostatic repulsion.
Podocyte slits create a final physical barrier to prevent leakage.
If proteins appear in urine, this indicates damage to the filtration barrier, as seen in kidney disease.
Active transport in the PCT depends on ATP to drive the sodium–potassium pumps that maintain the sodium gradient.
When ATP production decreases (for example, in low oxygen conditions):
The sodium gradient collapses, halting co-transport of glucose and amino acids.
Reabsorption efficiency falls, leading to glucose in urine (glycosuria).
Water reabsorption by osmosis is also reduced, increasing urine volume.
This demonstrates how metabolic energy is essential for kidney function.
