
Edexcel Syllabus focus:
'Know the benefits and risks of CVD treatments, including antihypertensives, statins, anticoagulants and platelet inhibitors.'
Drug treatments for cardiovascular disease lower the chance of damaging events such as heart attack or stroke, but each therapy has limits, side effects, and bleeding or metabolic risks that must be balanced carefully.
Why drug treatments are used
Cardiovascular drug treatments aim to reduce the chance of serious events by changing one or more major risk factors: blood pressure, blood cholesterol, or the tendency of blood to form harmful clots. Their main advantage is that they can lower risk over long periods without invasive procedures. Their main disadvantage is that they alter normal body processes, so side effects, interactions, and monitoring may be important.
Antihypertensives
High blood pressure increases the force exerted on artery walls and makes the heart work harder. Antihypertensives are prescribed to bring blood pressure down.
Antihypertensives: Drugs that lower blood pressure.
Different antihypertensive drugs act in different ways, for example by widening blood vessels, reducing heart rate, or increasing the loss of water and salts in urine. The overall biological effect is reduced pressure within the circulation.
Benefits of antihypertensives
Lower blood pressure reduces stress on artery walls.
This lowers the risk of events such as stroke, heart attack, and other complications linked to hypertension.
Reducing blood pressure can also decrease the workload of the heart, helping to protect cardiac tissue over time.
Risks of antihypertensives
Blood pressure may fall too much, causing dizziness, weakness, or fainting.
Some patients experience headaches, tiredness, or postural hypotension, where blood pressure drops when standing up.
Diuretic-type antihypertensives can disturb water balance or ion balance.
Not all patients respond equally well, so the first drug chosen may not be the most effective.
Statins
Statins are used when lowering blood cholesterol is an important part of reducing cardiovascular risk.
Statins: Drugs that reduce cholesterol production, mainly in the liver.
Statins lower the amount of cholesterol made by the body, often reducing LDL cholesterol.
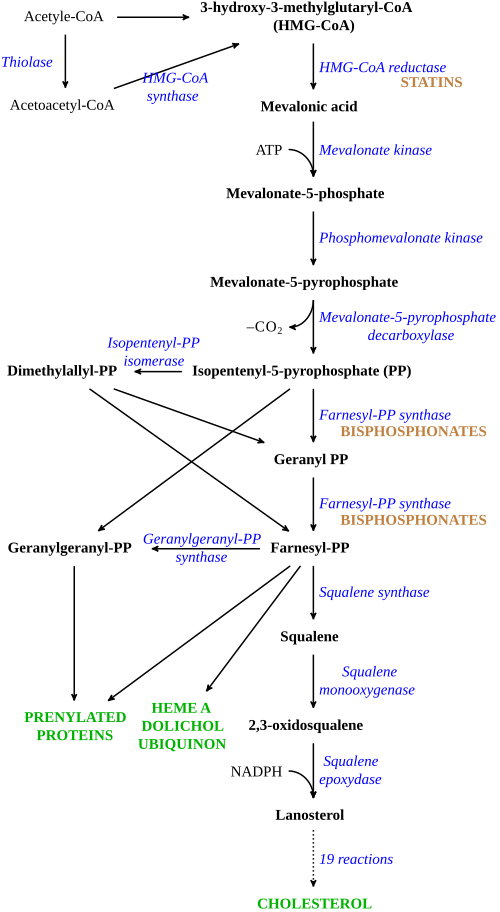
This pathway diagram summarizes the main steps of cholesterol biosynthesis and highlights the HMG‑CoA reductase step targeted by statins. By inhibiting this rate-limiting reaction, statins reduce endogenous cholesterol synthesis, which helps lower circulating LDL cholesterol and slows atherosclerotic plaque development. Source
This helps slow the buildup of fatty material in arteries and reduces the likelihood of future cardiovascular events. They are especially useful as a long-term preventive treatment.
Benefits of statins
Lowering cholesterol reduces the risk of further narrowing of arteries.
This can reduce the chance of heart attack and stroke.
Statins can be effective even when the patient does not feel unwell, because they target future risk rather than immediate symptoms.
Risks of statins
Some people develop muscle pain or muscle weakness.
Statins may affect the liver, so liver function may need to be checked.
Mild digestive side effects can occur.
Benefits are usually greatest with regular long-term use, so poor adherence reduces their effectiveness.
Anticoagulants
Some patients have an increased risk of harmful blood clots forming within the circulation. Anticoagulants are used to reduce this risk.
Anticoagulants: Drugs that reduce the rate at which blood clots form.
Anticoagulants interfere with the clotting process, so fibrin clots form more slowly.
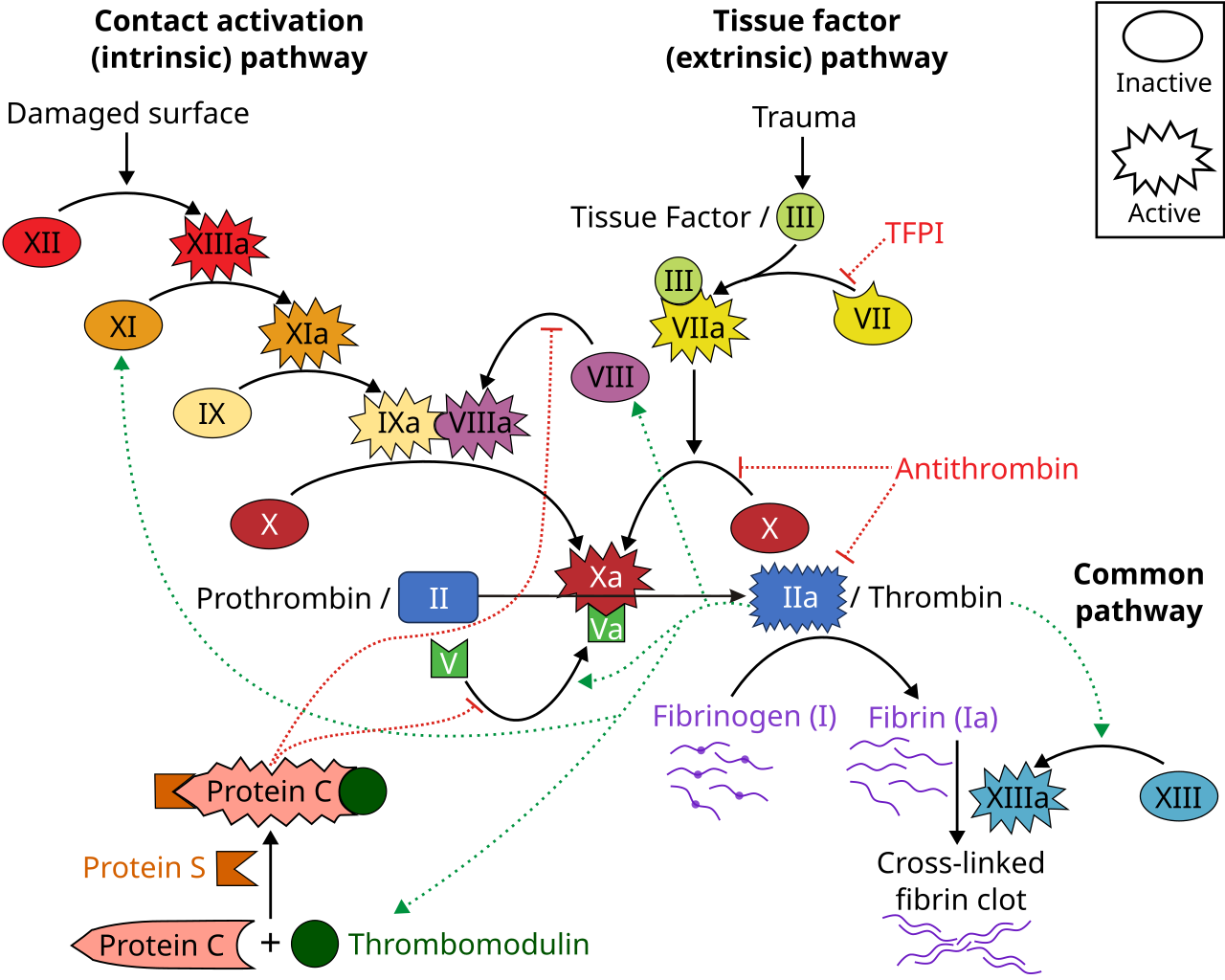
This diagram maps the coagulation cascade from the intrinsic and extrinsic pathways into the common pathway that produces thrombin and then fibrin. It helps explain how anticoagulants reduce clot formation by disrupting steps that lead to thrombin generation and fibrin polymer formation, which also clarifies why bleeding risk rises when clotting is suppressed. Source
They do not simply “thin” the blood; instead, they make the clotting response less likely to produce a dangerous blockage. Because clotting is also a normal protective response after injury, treatment must be carefully controlled.
Benefits of anticoagulants
Reduce the risk of dangerous clot formation.
Help prevent existing clots from getting larger.
Lower the likelihood of blocked blood vessels causing major tissue damage.
Risks of anticoagulants
The main risk is excessive bleeding.
Bleeding after an injury may last longer than normal.
Internal bleeding can occur and may not be immediately obvious.
Dose control may be important, because too little drug may not prevent clotting, but too much increases bleeding risk.
Platelet inhibitors
Some harmful clots begin when platelets stick together and form a platelet plug. Platelet inhibitors reduce this tendency.
Platelet inhibitors: Drugs that reduce platelet activation or platelet aggregation.
These drugs make platelets less likely to clump together at a damaged blood vessel wall.
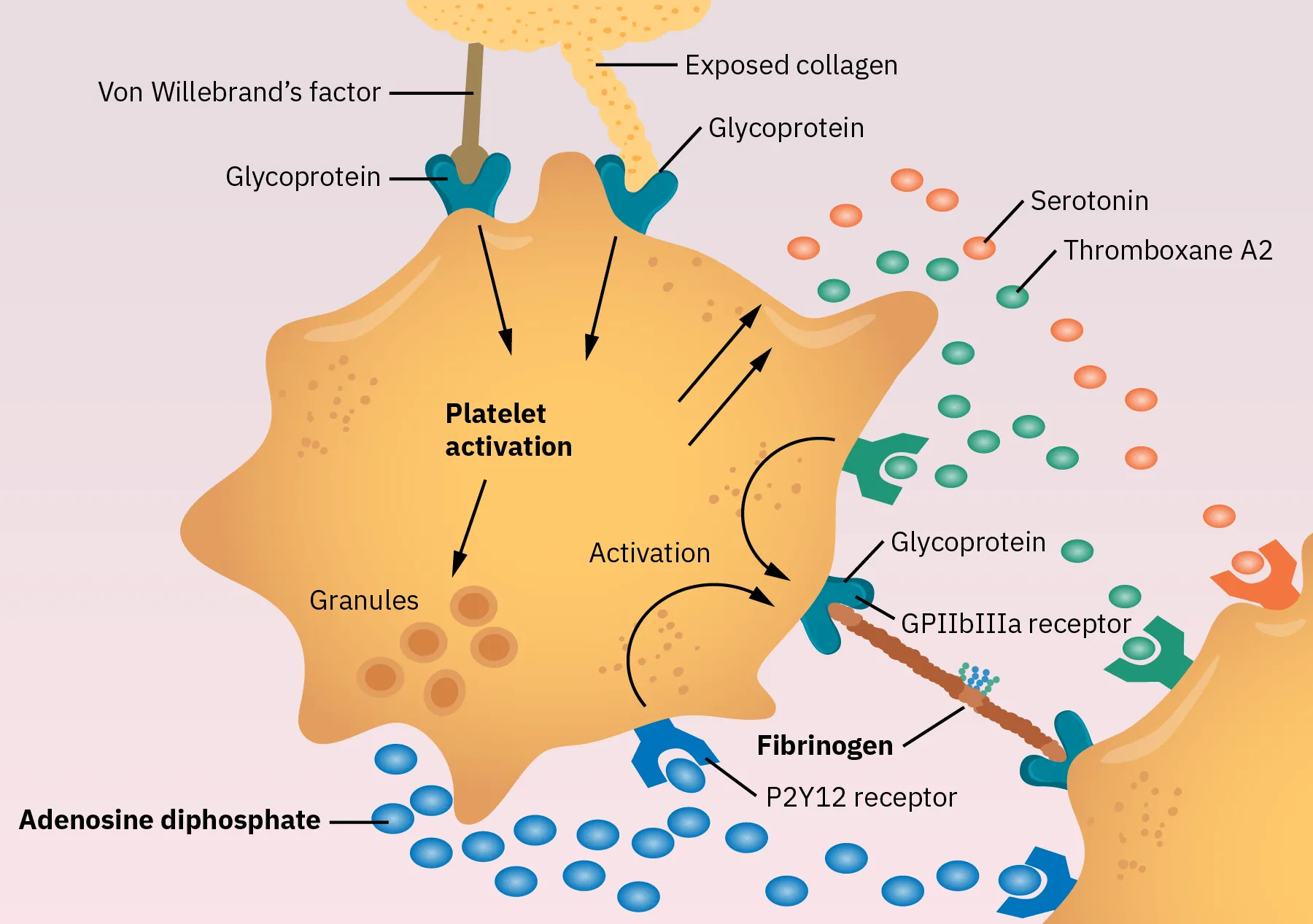
This schematic illustrates key chemical signals that activate platelets and promote platelet–platelet binding during primary hemostasis (platelet plug formation). It provides the mechanistic context for platelet inhibitors (e.g., aspirin), which reduce platelet activation pathways and therefore decrease inappropriate platelet aggregation in arteries. Source
A common example is aspirin, although other platelet inhibitors may also be prescribed. They are especially useful where the risk comes from unwanted platelet clumping in arteries.
Benefits of platelet inhibitors
Reduce the chance of platelets forming a harmful clot.
Lower the risk of arterial blockage leading to heart attack or stroke.
Can be used as long-term preventive treatment in some patients.
Risks of platelet inhibitors
Increase the risk of bleeding, especially after injury.
Aspirin can irritate the stomach lining and may increase the risk of ulcers.
Some patients cannot tolerate certain platelet inhibitors because of side effects or allergy.
Balancing benefit and risk
The most appropriate treatment depends on the patient’s individual risk factors, medical history, and other medications. Some people may need only one type of drug, while others may need a combination, such as a statin with an antihypertensive. Combination therapy can reduce cardiovascular risk more effectively because it targets different causes of disease.
However, using several drugs together also increases the chance of side effects and interactions. This is especially important when drugs that reduce clotting are combined, because bleeding risk rises. When judging any CVD treatment, the key issue is whether the reduction in future cardiovascular risk is greater than the harm that the treatment itself might cause.
Practice Questions
State one benefit and one risk of taking platelet inhibitors as a treatment for cardiovascular disease. (2 marks)
1 mark for one benefit, for example:
reduces platelet aggregation
reduces risk of clot formation
reduces risk of heart attack or stroke
1 mark for one risk, for example:
increased bleeding
stomach irritation
increased risk of ulcers
Explain how antihypertensives, statins, anticoagulants, and platelet inhibitors reduce cardiovascular disease risk. Include one possible disadvantage of any two of these treatments. (6 marks)
1 mark: antihypertensives lower blood pressure
1 mark: lower blood pressure reduces stress on artery walls / reduces workload of heart / lowers risk of cardiovascular events
1 mark: statins lower cholesterol production / lower blood cholesterol
1 mark: anticoagulants reduce the rate of clot formation / reduce fibrin clot formation
1 mark: platelet inhibitors reduce platelet activation or aggregation
1 mark: disadvantages of any two treatments, for example:
antihypertensives may cause dizziness or fainting
statins may cause muscle pain or affect the liver
anticoagulants increase bleeding risk
platelet inhibitors increase bleeding risk or may irritate the stomach
FAQ
Some anticoagulants, such as warfarin, can be strongly affected by diet, illness, and other medicines. That means their effect can vary a lot between patients and over time.
Regular blood tests help check whether clotting is being reduced enough to prevent harmful clots, but not so much that dangerous bleeding occurs. Newer anticoagulants usually have more predictable effects, so routine testing is often less frequent.
The liver often makes more cholesterol at night. Taking certain statins in the evening can therefore improve how well they reduce cholesterol production.
This matters most for shorter-acting statins. Longer-acting statins may still work well even if taken at a different time, as long as they are taken consistently and according to medical advice.
At low doses, aspirin is mainly used because it reduces platelet activity. That makes it useful for lowering the risk of unwanted clot formation in some patients.
At higher doses, aspirin also acts more strongly as a painkiller and anti-inflammatory drug. The dose matters because the benefit being targeted is different, and higher doses can increase side effects.
Different antihypertensive classes work by different mechanisms, so one type may suit a patient better than another. Increasing the dose of the first drug may give more side effects without enough extra benefit.
Doctors may switch drugs if blood pressure stays high, if side effects are troublesome, or if another medical condition makes a different drug more appropriate.
Many CVD drugs are preventive. They reduce future risk even when a person feels completely well, so the absence of symptoms does not mean the risk has disappeared.
Stopping treatment suddenly may allow blood pressure, cholesterol, or clotting risk to rise again. In some cases, this can quickly increase the chance of a serious event such as a heart attack or stroke.

{kind=link}
{kind=link}