
OCR Specification focus:
‘Describe the principles and potential of gene therapy, distinguishing between somatic cell and germ line approaches.’
Gene therapy aims to treat or prevent genetic disorders by introducing functional genes into cells, offering long-term solutions by correcting underlying genetic defects at their source.
Principles of Gene Therapy
Gene therapy is the medical technique that involves the introduction, removal, or alteration of genetic material within a person’s cells to treat or prevent disease. Its main goal is to replace faulty alleles with functional ones to restore normal cellular function. The process typically uses vectors, most commonly modified viruses, to deliver therapeutic DNA into target cells.
The Need for Gene Therapy
Many diseases result from mutations in a single gene that cause a non-functional or missing protein. Traditional treatments often address only the symptoms, but gene therapy targets the root genetic cause, providing the potential for long-lasting or permanent correction.
Core Stages of Gene Therapy
The general stages of gene therapy involve several key steps:
Identification of the target gene responsible for the condition.
Production of a functional copy of this gene in the laboratory.
Selection of an appropriate vector, often a modified virus such as a retrovirus, adenovirus, or liposome.
Delivery of the vector to the patient’s target cells either directly (in vivo) or indirectly (ex vivo).
Expression of the new gene, allowing the synthesis of the correct protein and restoration of normal cell function.
The success of gene therapy depends on stable gene expression, correct cellular targeting, and minimal immune rejection.
Vectors and Delivery Methods
Vectors are essential carriers that transport the therapeutic gene into host cells.
Vector: A vehicle used to transfer genetic material into a target cell, often derived from viruses or synthetic systems such as liposomes.
Common types of vectors include:
Retroviral vectors – integrate their genetic material into the host genome, providing long-term expression but posing a small risk of insertional mutagenesis.
Adenoviral vectors – deliver DNA to the nucleus without integrating into the host genome, allowing temporary expression suitable for non-dividing cells.
Adeno-associated viruses (AAVs) – low pathogenicity and relatively stable expression; increasingly favoured in clinical applications.
Non-viral methods – use liposomes or naked plasmid DNA; safer but less efficient.
Delivery can occur through:
In vivo therapy – direct injection of the vector into the patient’s body.
Ex vivo therapy – cells are removed from the patient, genetically modified in a laboratory, and then reintroduced.
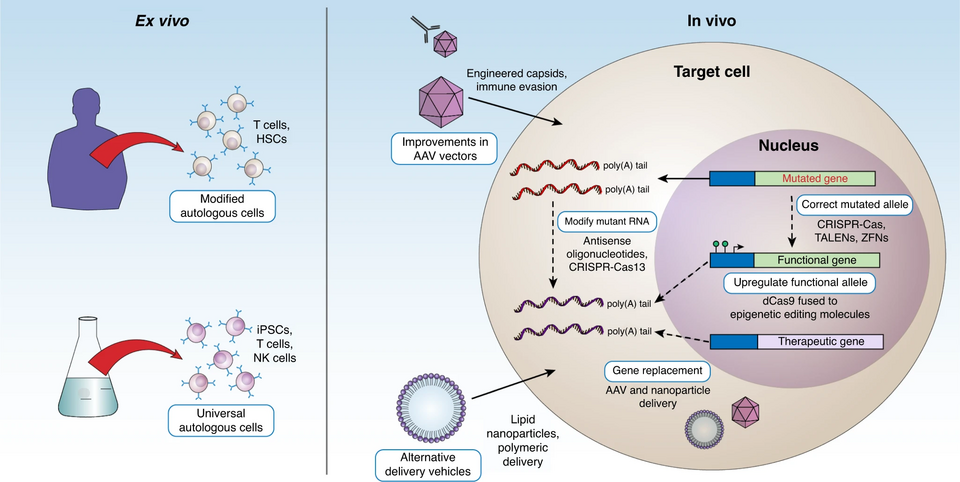
Two-panel schematic comparing ex vivo (left) and in vivo (right) gene therapy. It highlights cell removal and modification outside the body versus direct delivery to target tissues, aligning with standard workflows used in somatic therapies. The image includes brief labels on vectors and targeting but no extraneous detail beyond what is covered in the notes. Source.
Types of Gene Therapy: Somatic vs Germ Line
Somatic Cell Gene Therapy
Somatic cell gene therapy targets non-reproductive cells of the body. Any genetic modifications affect only the treated individual and are not inherited by offspring.
Somatic Cell Gene Therapy: Genetic modification of body (somatic) cells to correct a disease phenotype without affecting the patient’s gametes or future generations.
Key characteristics:
Only affects the treated tissues or organs.
Must be repeated if cells have limited lifespan or the gene is not permanently integrated.
Considered ethically acceptable and widely researched.
Examples include:
Cystic fibrosis – insertion of a functional CFTR gene into lung epithelial cells using liposomes or viral vectors.
Haemophilia – delivery of the gene for clotting factor IX to liver cells.
Severe Combined Immunodeficiency (SCID) – correction of defective ADA or IL2RG genes in immune system cells.
Advantages:
Targets disease at its genetic origin.
Non-heritable changes prevent long-term genetic alterations in the human population.
Potential to provide a cure rather than symptomatic treatment.
Limitations:
Temporary effect if the vector DNA is not integrated.
Difficult to target all affected cells in large organs.
Immune response to viral vectors can reduce effectiveness or cause side effects.
Germ Line Gene Therapy
Germ line gene therapy involves the modification of gametes (sperm or ova) or zygotes, introducing genetic changes that are heritable by all future generations of the individual.
Germ Line Gene Therapy: The alteration of genes in reproductive cells or early embryos so that the genetic modification is inherited by offspring.
This method has the potential to permanently eliminate genetic disorders from a family lineage. However, it also carries significant ethical, legal, and technical concerns.
Potential benefits include:
Prevention of inherited genetic diseases such as Duchenne muscular dystrophy or Huntington’s disease.
Long-term population health benefits if deleterious alleles are removed.
Risks and challenges:
Unintended mutations may arise due to off-target effects.
Ethical issues concerning consent (future generations cannot consent).
Fear of “designer babies” and social inequality based on genetic modification.
Currently banned in humans in most countries under international agreements such as the Oviedo Convention.
Principles Underpinning Both Approaches
Both somatic and germ line gene therapies rely on understanding the genetic basis of disease, identifying target sequences, and ensuring safe and efficient gene delivery. The process requires bioinformatics for accurate gene sequencing, as well as synthetic biology to engineer compatible vectors and regulatory elements.
Bioinformatics: The application of computational tools to manage and analyse biological data, especially genetic sequences.
In practice, both approaches are underpinned by genome sequencing and molecular cloning technologies, allowing scientists to isolate, copy, and modify genes precisely. Emerging tools such as CRISPR–Cas9 have revolutionised gene editing by providing highly specific DNA targeting and modification, offering the potential for both safe somatic treatments and, in theory, germ line correction.
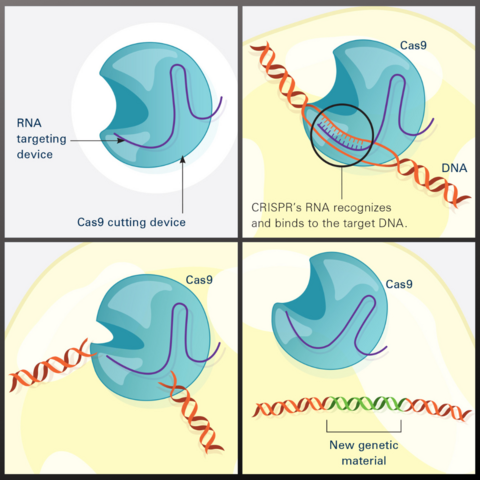
Illustrated sequence of CRISPR–Cas9 editing: guide RNA targets the DNA sequence, Cas9 creates a double-strand break, and repair incorporates the desired change. This diagram focuses on the essential stages needed to understand how editing underpins gene therapy and omits research-level complexities beyond the syllabus. Source.
Potential and Future Directions
While somatic therapy remains the focus of current clinical practice, advances in vector technology, CRISPR systems, and epigenetic regulation continue to improve safety and precision. Research aims to achieve controlled expression of therapeutic genes and minimise immune reactions.
Ethical discourse continues around germ line modification, balancing potential health benefits against concerns about human genetic diversity and equity. The long-term vision of gene therapy remains the eradication of inherited disease, but it demands stringent oversight and a deep understanding of the molecular and societal implications.
Practice Questions
Question 1 (2 marks)
Explain the difference between somatic cell gene therapy and germ line gene therapy.
Mark scheme:
1 mark for correctly identifying that somatic cell gene therapy affects body (non-reproductive) cells only and changes are not inherited.
1 mark for correctly identifying that germ line gene therapy affects gametes or embryos and changes are heritable by offspring.
Question 2 (5 marks)
Discuss the ethical and practical issues associated with using germ line gene therapy in humans.
Mark scheme:
Award up to 5 marks for the following indicative points (maximum 1 mark per point):
Potential to eliminate inherited genetic disorders permanently from family lines (benefit).
Ethical issue of lack of consent from future generations.
Concern over “designer babies” or enhancement beyond therapy (ethical risk).
Risk of off-target mutations or unintended effects (practical/technical limitation).
Current legal restrictions or bans on germ line modification in humans (contextual awareness).
Credit any other relevant and accurate ethical or technical points supported with biological understanding.
FAQ
Viral vectors used in gene therapy are genetically engineered to remove pathogenic genes, preventing them from causing disease. The remaining viral genome retains only the essential sequences for entry into host cells and gene delivery.
In addition:
Replication genes are deleted so the virus cannot multiply in the patient.
Control sequences are inserted to regulate expression of the therapeutic gene.
The vectors are often produced in laboratory cell lines that supply the missing viral proteins, ensuring safety outside the production environment.
This ensures high efficiency with minimal risk of infection or unintended gene activation.
Introducing a functional gene is only the first step; its expression level must be controlled for therapeutic success.
If expression is too low, the therapy fails to correct the condition. If too high, it can disrupt normal cell metabolism. Scientists use:
Promoter sequences to control transcription rates.
Tissue-specific promoters to restrict expression to target cells.
Regulatory elements such as enhancers and silencers to fine-tune gene activity.
Effective regulation prevents toxicity and ensures sustained, physiologically appropriate protein production.
Targeting accuracy is crucial to avoid side effects and maximise therapeutic benefit. Challenges include:
Reaching the target tissue through biological barriers (e.g. blood–brain barrier, mucosal layers).
Ensuring uptake by the correct cell type without immune clearance.
Achieving stable integration into the genome or long-term persistence in non-dividing cells.
Solutions involve using cell-specific promoters, targeted viral envelopes, or nanoparticle coatings that guide the vector precisely to intended cells.
After administration, patients undergo careful molecular and clinical monitoring to confirm gene expression and detect any adverse effects.
Key checks include:
PCR and sequencing to confirm insertion of the therapeutic gene.
Protein assays to measure expression of the desired product.
Immunological testing to detect inflammatory or allergic responses.
Long-term follow-up to monitor for oncogenic effects or loss of function.
These assessments ensure the therapy remains both effective and safe over time.
Yes, CRISPR–Cas9 could theoretically edit defective alleles in embryos or gametes, offering permanent correction of genetic diseases.
However, it is controversial because:
Off-target mutations might cause unintended damage in the genome.
Future generations would inherit any errors.
It raises ethical concerns about human enhancement and the definition of acceptable genetic change.
Currently, international guidelines prohibit germ line editing in humans, allowing only basic research under strict ethical supervision
