
Edexcel Syllabus focus:
'Know the evidence for a causal relationship between blood cholesterol levels, including total cholesterol and LDL cholesterol, and CVD.'
Researchers do not treat cholesterol and cardiovascular disease as linked by coincidence alone. The strongest judgment comes from several independent lines of evidence that point to cholesterol, especially LDL cholesterol, as a cause of disease.
Causation and not just association
When scientists link cholesterol to cardiovascular disease (CVD), they mean more than a statistical pattern. They ask whether raised cholesterol appears before disease, whether risk rises as cholesterol rises, whether the same pattern is found in many studies, and whether lowering cholesterol reduces disease.
Causal relationship: A relationship in which a change in one factor directly contributes to a change in another factor, rather than the two factors only being associated.
A single study cannot prove causation by itself. People with high cholesterol may also differ in diet, physical activity, smoking, body mass, or age. These are confounding variables, so strong conclusions need multiple types of evidence that all point in the same direction.
Why timing matters
For a factor to be causal, exposure must come before the outcome. Prospective cohort studies are useful because cholesterol is measured first, then participants are followed for years to see who develops heart attacks, strokes, or other CVD events. This makes reverse causation less likely, because the disease has not already occurred when cholesterol is measured.
Observational evidence linking cholesterol and CVD
Large observational studies have shown that people with higher blood cholesterol tend to have higher rates of CVD. This applies to total cholesterol, but it is especially clear for LDL cholesterol.
Important patterns in the evidence include:
a positive association between blood cholesterol and CVD risk
a dose-response relationship, where higher LDL levels are linked to higher risk
consistency across different countries, age groups, and study designs
repeated findings in very large populations, which makes chance less likely
These patterns matter because causal factors often show a graded effect. If rising LDL is followed by rising CVD risk, that supports the idea that LDL is involved in the disease process rather than simply being an unrelated marker.
There is also biological plausibility. LDL can enter artery walls and contribute to plaque formation, which makes the statistical association more convincing as a causal one.
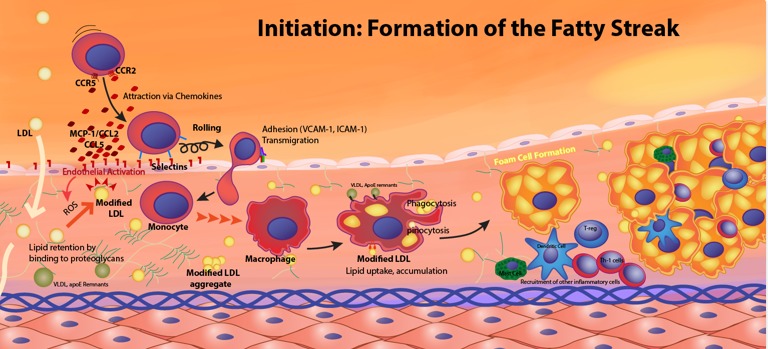
Initiation of atherosclerosis (fatty streak formation): LDL particles are retained beneath the endothelium, can become modified, and promote recruitment of monocytes that differentiate into macrophages. Macrophages take up modified LDL and become foam cells, creating an early lipid-rich lesion in the artery wall. This connects raised LDL to a concrete disease mechanism rather than a purely statistical association. Source
LDL cholesterol: Cholesterol carried in low-density lipoproteins; high levels are strongly associated with increased risk of cardiovascular disease.
Genetic evidence
Another strong line of evidence comes from inherited conditions that produce very high LDL cholesterol from a young age. People with these conditions often develop CVD much earlier than expected. This is important because their raised LDL is present for many years, often before adult lifestyle factors could explain the difference.
Genetic evidence is powerful for two reasons:
it reduces the likelihood that the association is caused only by lifestyle confounders
it shows that long-term exposure to high LDL increases lifetime CVD risk
This supports the idea that LDL is not just linked to disease, but helps drive the disease process.
Intervention evidence
Some of the strongest evidence for causation comes from studies in which LDL cholesterol is deliberately lowered and disease outcomes are then measured. In randomized controlled trials, lowering LDL reduces the number of CVD events.
This matters because experimental evidence tests the factor directly:
if LDL were only an innocent marker, lowering it would not be expected to reduce disease consistently
if lowering LDL leads to fewer heart attacks or strokes, that supports a cause-and-effect relationship
The evidence is stronger when larger reductions in LDL are associated with larger reductions in risk. This again supports a dose-response pattern. It also shows that the relationship is not based only on observation; it is supported by intervention.
Total cholesterol and LDL cholesterol
Total cholesterol is still useful, because raised total cholesterol is often associated with increased CVD risk. However, total cholesterol is a broader measure and is less specific than LDL. Two people may have the same total cholesterol but different amounts of LDL cholesterol.
Because of this, evidence based specifically on LDL cholesterol is often more convincing than evidence based on total cholesterol alone. LDL is more directly linked to the disease process, so it gives a clearer picture of causal risk.
Interpreting causation in biology
Biological causation does not mean certainty. Not every person with high LDL develops CVD early, and some people with lower LDL still develop disease. That does not weaken the causal case. In biology, a causal factor often changes probability of disease, not whether disease happens in every individual.
Scientists therefore judge the cholesterol-CVD relationship by weighing several features together:
association in observational studies
temporal sequence, with cholesterol measured before disease develops
dose-response relationships
biological plausibility
genetic evidence from inherited high LDL
experimental evidence showing that lowering LDL reduces CVD events
This is why the evidence for a causal relationship is much stronger than a simple correlation, especially for LDL cholesterol.
Practice Questions
State two pieces of evidence that support a causal relationship between raised LDL cholesterol and CVD. (2 marks)
1 mark for stating that higher LDL is associated with higher CVD risk in observational studies
1 mark for stating that lowering LDL reduces CVD events in intervention or randomized trials
1 mark for stating that risk increases as LDL increases (dose-response)
1 mark for stating that inherited very high LDL is linked to early CVD
Max 2 marks
Explain why scientists conclude that raised LDL cholesterol has a causal role in CVD rather than being only correlated with it. (6 marks)
Higher LDL is associated with higher CVD risk in large studies (1)
LDL is measured before disease develops in prospective studies, so timing supports causation (1)
The same pattern is found repeatedly in different populations or studies (1)
There is a dose-response relationship, with higher LDL linked to greater risk (1)
LDL has a biologically plausible role because it contributes to plaque formation in arteries (1)
Lowering LDL reduces the number of CVD events in trials, supporting cause and effect (1)
FAQ
ApoB is a protein found on the surface of each major atherogenic lipoprotein particle. Because each particle usually carries one ApoB molecule, ApoB gives an estimate of the number of particles, not just how much cholesterol they contain.
In some people, particle number may predict risk more accurately than LDL cholesterol concentration, especially when cholesterol content per particle varies.
LDL is an important causal factor, but it is not the only influence on disease risk.
Other contributors include:
blood pressure
smoking
diabetes
inflammation
genetics
duration of exposure to cholesterol over time
So a “normal” LDL result does not mean zero risk. It means that one major risk factor is lower, not absent.
Yes. CVD risk depends not only on the LDL level at one moment, but also on cumulative exposure over many years.
A person with moderately raised LDL for decades may have greater long-term risk than someone whose LDL rises later in life. This is one reason early detection matters when researchers interpret cholesterol-related risk.
In many labs, LDL is estimated from other blood results because it is faster and cheaper than direct measurement.
Calculated LDL is usually reliable when triglyceride levels are not very high. If triglycerides are elevated, or if the result seems inconsistent with the clinical picture, a direct LDL measurement may be more useful.
Total cholesterol and LDL usually change only a little after eating, so a nonfasting sample is often good enough for routine risk assessment.
The main exception is when triglycerides are important, because they can rise more noticeably after meals. If triglycerides are unusually high, a fasting repeat sample may be requested for clearer interpretation.
