
Edexcel Syllabus focus:
'Understand how scientific knowledge about diet, obesity indicators, BMI, waist-to-hip ratio, exercise and smoking can reduce coronary heart disease risk.'
Coronary heart disease risk can often be lowered by informed lifestyle choices. Biology explains how diet, body fat distribution, physical activity, and smoking influence the condition of the coronary arteries.
Diet and coronary heart disease risk
Diet affects several major CHD risk factors, including blood cholesterol, blood pressure, and body mass. This means that improving diet can reduce the chance of coronary arteries becoming narrowed.
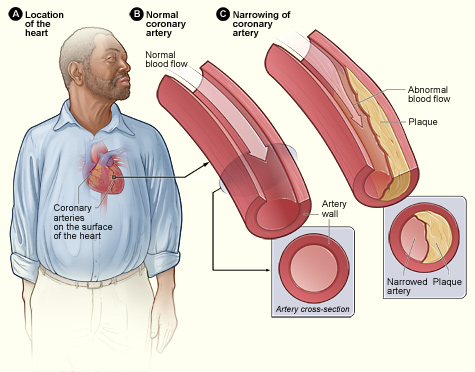
Diagram of a normal coronary artery compared with an artery narrowed by atherosclerotic plaque. It highlights how plaque buildup reduces lumen diameter and therefore limits blood flow through the coronary circulation. Source
A diet high in saturated fat is linked to higher levels of LDL cholesterol in the blood. Higher LDL levels increase the likelihood of fatty material being deposited in artery walls. Reducing saturated fat intake, and replacing some of it with unsaturated fats, can therefore help reduce CHD risk.
Diet also affects blood pressure. Eating too much salt can contribute to high blood pressure, which places extra stress on artery walls and increases the chance of damage. Lower salt intake can help reduce this strain.
Energy intake matters as well. If a person regularly consumes more energy than they use, the excess is stored, leading to weight gain and possible obesity. This raises CHD risk. Scientific understanding of nutrition therefore supports:
reducing excess saturated fat
avoiding excessive salt intake
keeping energy intake balanced with energy expenditure
choosing foods that support a healthy body mass
These changes are most effective when they are long term rather than short-term dieting.
Obesity indicators and coronary heart disease risk
Obesity is strongly associated with increased CHD risk. However, risk is not determined only by total body mass. The distribution of fat is also important, because fat stored around the abdomen is more strongly linked to cardiovascular disease than fat stored elsewhere.
For this reason, scientists use obesity indicators such as BMI and waist-to-hip ratio. These measurements do not diagnose CHD, but they help identify people whose risk is higher and who may benefit from lifestyle changes.
BMI
BMI is widely used as a simple estimate of whether body mass is appropriate for height.
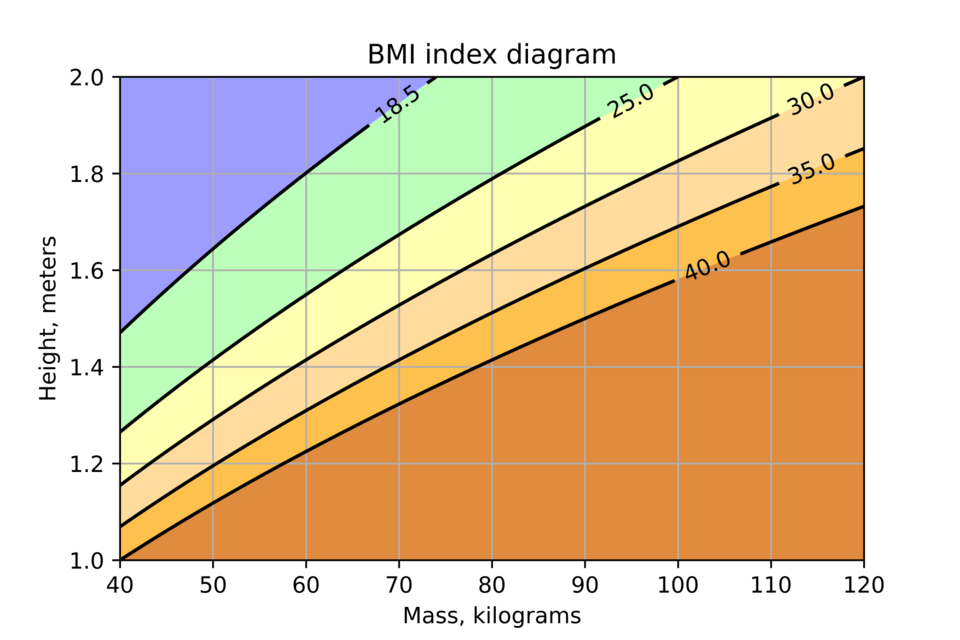
BMI classification diagram showing the relationship and the standard category cut-offs (underweight, normal, overweight, and obesity classes). This supports how BMI is used as a quick screening indicator when comparing individuals or populations. Source
BMI: Body mass index, an obesity indicator calculated from a person's mass and height to estimate whether their body mass is within a healthy range.
BMI is useful because it is quick, inexpensive, and suitable for comparing large populations. In general, a higher BMI is associated with greater CHD risk because it often reflects excess body fat.
Insert example content here...
= body mass in kilograms, kg
= height in meters, m
A BMI in the healthy range suggests lower risk than a BMI in the obese range. However, BMI has important limitations. It does not distinguish between fat mass and muscle mass, so a very muscular person may have a high BMI without excess fat. It also gives no information about where fat is stored.
Waist-to-hip ratio
Because fat distribution matters, waist-to-hip ratio can sometimes be more useful than BMI when assessing CHD risk.
Waist-to-hip ratio: An obesity indicator found by dividing waist circumference by hip circumference to estimate how much fat is stored around the abdomen compared with the hips.
A higher ratio suggests more central obesity, meaning a greater proportion of fat is stored around the waist. This pattern is more closely linked to CHD risk than general body mass alone.
= waist circumference in centimeters or meters
= hip circumference in the same unit
Waist-to-hip ratio is valuable because it gives information that BMI cannot. Two people may have the same BMI, but the person with the higher waist-to-hip ratio may be at greater risk. For this reason, BMI and waist-to-hip ratio are often best used together.
Exercise and reducing risk
Regular exercise reduces CHD risk through several biological effects. It helps maintain a healthy energy balance, so it can reduce body fat and lower both BMI and waist-to-hip ratio over time.
Exercise can also:
lower blood pressure
improve the balance of blood lipids, including increasing HDL cholesterol
improve cardiovascular efficiency
reduce the likelihood of obesity developing
The benefit comes from regular physical activity rather than occasional intense exercise. Scientific evidence therefore supports exercise as an important lifestyle change for lowering coronary heart disease risk.
Smoking and reducing risk
Smoking is a major modifiable risk factor for CHD, meaning it is something a person can change.
Modifiable risk factor: A factor that affects disease risk and can be reduced or changed by behavior or lifestyle choice.
Chemicals in tobacco smoke damage the endothelium lining the arteries. This makes the artery wall more likely to become diseased. Smoking also increases blood pressure and makes the heart work harder. In addition, smoking increases the tendency of the blood to clot, which raises the risk of a coronary artery becoming blocked.
Stopping smoking therefore reduces CHD risk because it:
reduces further damage to artery walls
lowers blood pressure and heart strain
decreases the chance of clot formation
improves overall cardiovascular health over time
Scientific knowledge has shown that avoiding smoking, or quitting if already smoking, is one of the most effective ways to lower coronary heart disease risk.
Using measurements to guide risk reduction
BMI and waist-to-hip ratio are useful because they allow progress to be monitored during lifestyle change. If diet improves and exercise increases, these indicators may move toward healthier values. This helps show whether interventions are likely to reduce CHD risk.
They should be seen as screening tools, not perfect measures. Even so, when combined with knowledge about diet, exercise, and smoking, they provide a practical way to identify risk and support prevention.
Practice Questions
Explain one limitation of BMI as an indicator of coronary heart disease risk. (2 marks)
BMI does not distinguish between fat mass and muscle mass. (1)
Therefore a muscular person may have a high BMI without having excess body fat or the same CHD risk. (1)
Explain how scientific knowledge about diet, obesity indicators, exercise, and smoking can be used to reduce coronary heart disease risk. (6 marks)
Award 1 mark for each correct point, up to 6 marks:
reducing saturated fat intake can lower LDL cholesterol
reducing salt intake can help lower blood pressure
balancing energy intake with energy expenditure can reduce weight gain or obesity
BMI can be used to estimate whether body mass is in a healthy range
waist-to-hip ratio can identify central obesity, which is linked to higher CHD risk
regular exercise can reduce body fat
regular exercise can lower blood pressure
regular exercise can improve blood lipid profile, for example by increasing HDL
smoking damages artery lining or endothelium
smoking increases blood pressure or heart workload
stopping smoking reduces further arterial damage
stopping smoking reduces the risk of clot formation
FAQ
BMI only uses mass and height, so it cannot show body composition or fat distribution.
Two people with the same BMI may differ because:
one has more muscle and less fat
one stores more fat around the abdomen
one has other lifestyle risks, such as smoking or inactivity
This is why BMI is more useful when combined with measures such as waist-to-hip ratio.
Abdominal fat, especially fat deep around the organs, is metabolically active.
It is associated with:
greater release of inflammatory chemicals
increased insulin resistance
less favorable blood lipid patterns
These effects make central obesity more strongly linked to coronary heart disease than fat stored mainly around the hips and thighs.
Some effects improve quite quickly, while others take longer.
Heart rate and blood pressure can begin to improve soon after smoking stops.
The tendency for blood to clot also starts to fall.
Damage already present in arteries does not disappear immediately, so long-term risk falls gradually rather than instantly.
The earlier someone quits, the greater the long-term benefit.
Both can help.
Aerobic exercise is especially effective for improving cardiovascular fitness, but strength training can also:
increase energy use
help maintain a healthy body mass
improve glucose control
support long-term activity levels
A balanced program that includes both types of exercise is often more sustainable and beneficial than relying on only one form.
Food labels can make risk reduction more practical by allowing better comparison between products.
They are especially useful for checking:
saturated fat content
salt content
calorie content per portion
portion size compared with the whole package
This helps people make more informed choices rather than relying only on advertising or assumptions about whether a food is “healthy.”

{kind=link}
{kind=link}