
Edexcel Syllabus focus:
'Know the cardiac cycle, including atrial systole, ventricular systole and cardiac diastole, and how heart structure and function can be investigated practically.'
Each heartbeat follows a precise pattern of contraction and relaxation. Understanding this sequence explains how blood is moved efficiently through the heart and how heart activity can be studied in the lab.
The cardiac cycle
The cardiac cycle is the repeating sequence of events in one heartbeat.
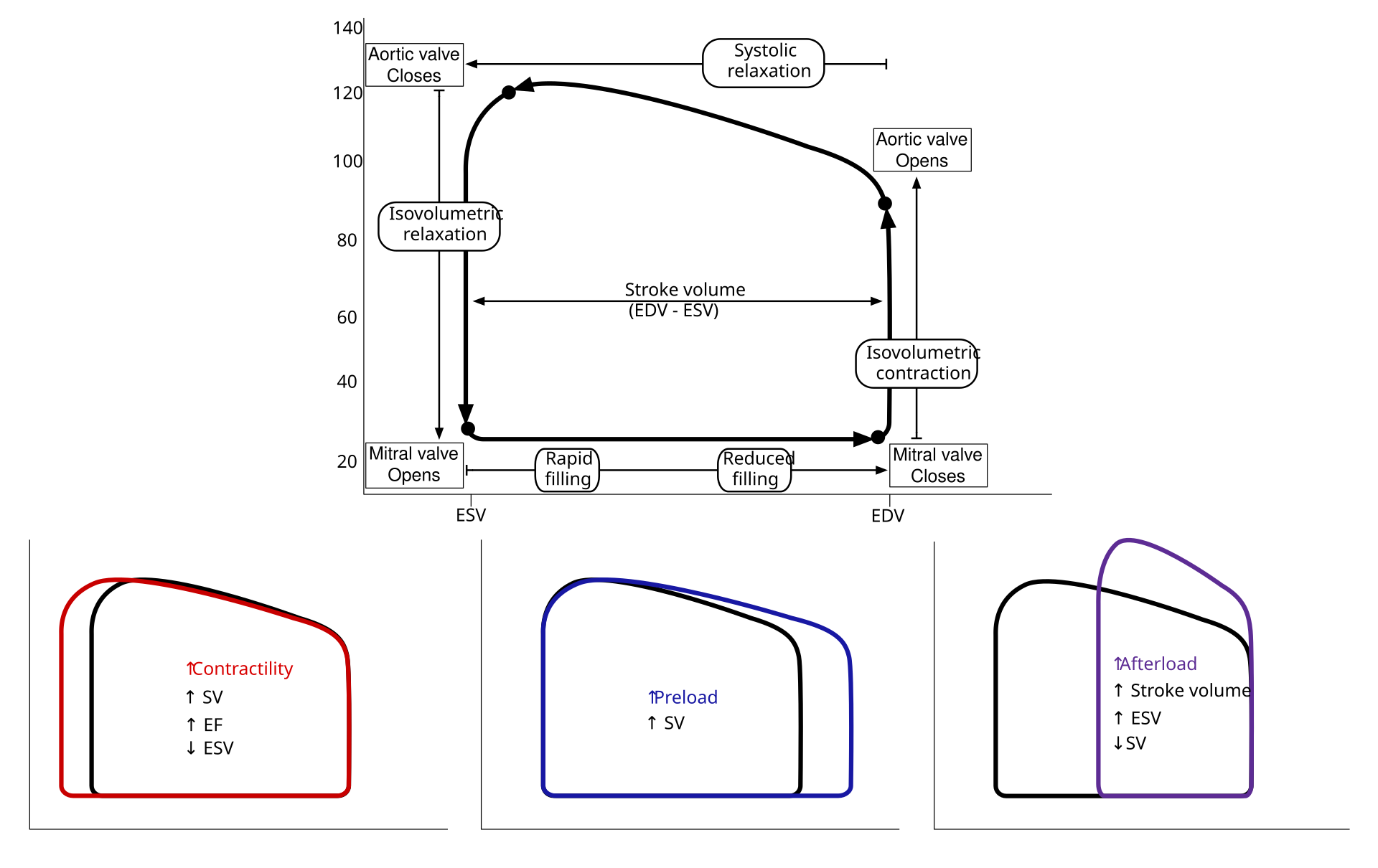
Pressure–volume loop for the left ventricle across one cardiac cycle, showing the sequence of filling, isovolumetric contraction, ejection, and isovolumetric relaxation. The loop makes it clear when ventricular pressure rises without a change in volume (valves closed) versus when volume changes during filling or ejection (valves open). This helps translate the worded phases (diastole/systole) into a quantitative pressure-based model. Source
It depends on changes in pressure inside the atria, ventricles, and connected arteries.
Cardiac cycle: One complete heartbeat, from the beginning of one beat to the beginning of the next.
The cycle keeps blood flowing in one direction because valves open when pressure behind them is greater than pressure in front of them, and close when the pressure difference reverses. The main phases named in the specification are cardiac diastole, atrial systole, and ventricular systole.
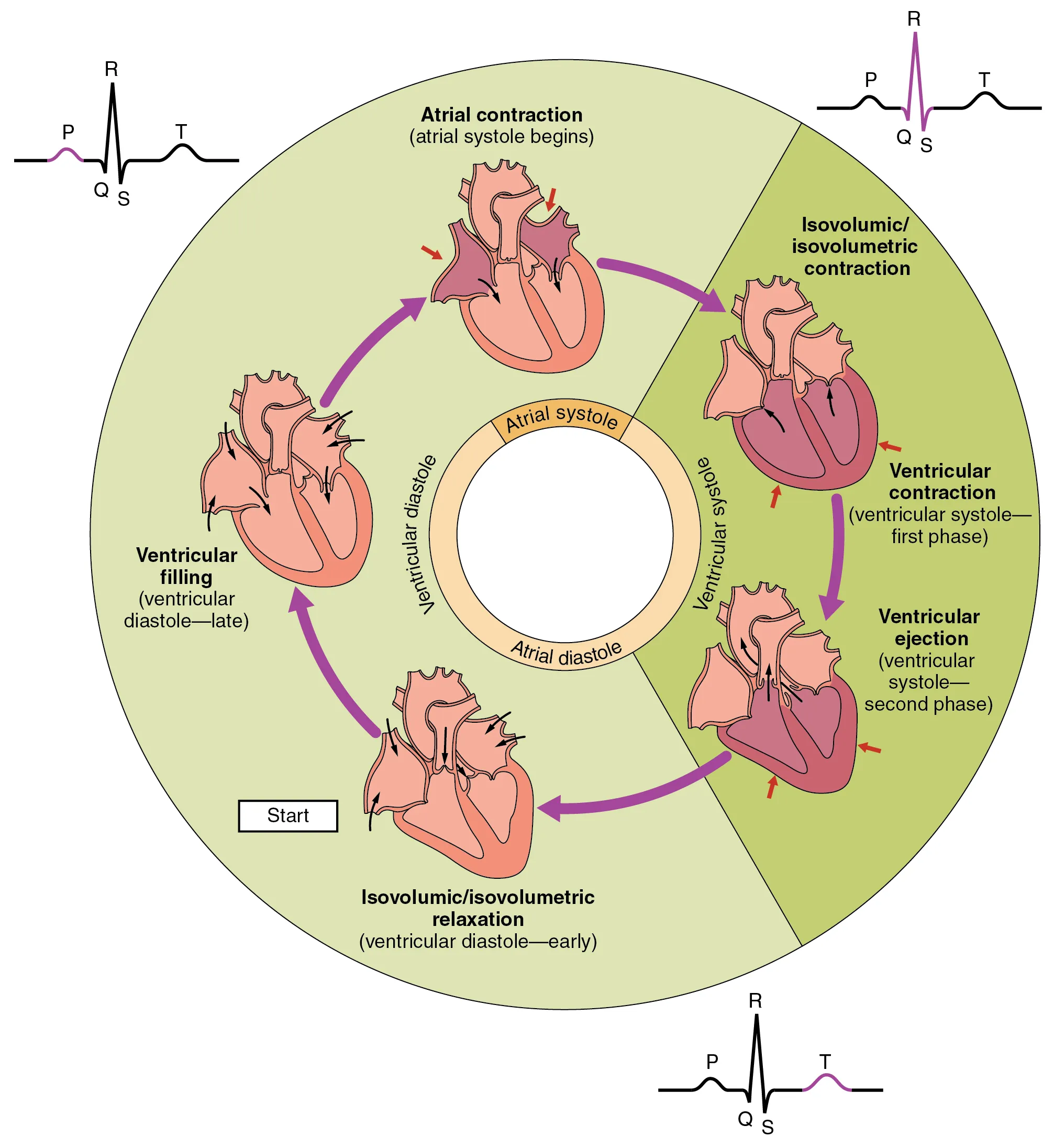
Teaching diagram summarizing the phases of the cardiac cycle and how atrial and ventricular events alternate across one heartbeat. It supports quick recall of the sequence (diastole → atrial systole → ventricular systole → return to diastole) and helps students map each named phase to what the chambers are doing. Use it as a high-level overview before adding detail with pressure/valve explanations. Source
Cardiac diastole
During cardiac diastole, both the atria and ventricles are relaxed. Blood returns to the heart from the veins, filling the atria and then moving into the ventricles.
Cardiac diastole: The relaxation phase of the heart, when chambers refill with blood.
At this stage:
pressure in the ventricles is low
pressure in the arteries is higher than in the ventricles, so the semilunar valves are closed
pressure in the atria becomes greater than in the ventricles, so the atrioventricular valves open
most ventricular filling happens passively, without the atria contracting
This passive filling is important because it means the heart does not need to use contraction for the whole filling process.
Atrial systole
Atrial systole is the contraction of the atria. This raises atrial pressure and pushes the last portion of blood into the ventricles. The atrioventricular valves remain open, and the semilunar valves remain closed because ventricular pressure is still lower than arterial pressure.
Atrial systole completes ventricular filling just before the ventricles contract. It is sometimes described as a “top-up” phase because much of the blood has already entered during diastole.
Ventricular systole
Ventricular systole is the contraction of the ventricles. As the ventricular walls contract, ventricular pressure rises rapidly. This causes the atrioventricular valves to close, which prevents blood from flowing back into the atria.
When ventricular pressure becomes greater than the pressure in the aorta and pulmonary artery:
the semilunar valves open
blood is forced out of the ventricles
the right ventricle sends blood to the lungs
the left ventricle sends blood to the body
After ejection, the ventricles begin to relax. Ventricular pressure falls, and when it drops below arterial pressure, the semilunar valves close. This prevents backflow from the arteries into the ventricles. The cycle then returns to cardiac diastole.
The closing of heart valves produces the familiar heart sounds:
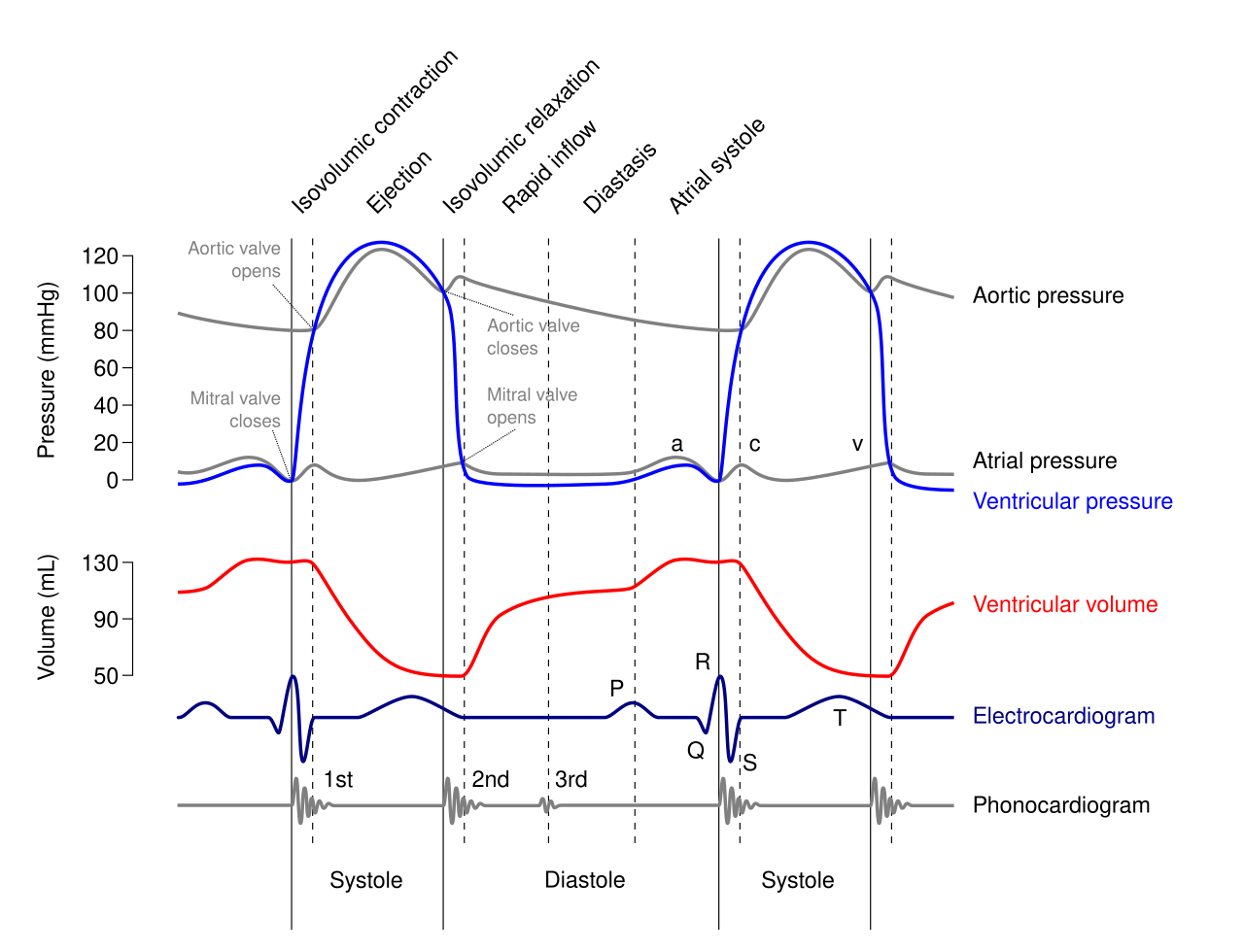
Wiggers diagram of the left heart showing how atrial/ventricular pressure changes align with ventricular volume, the ECG, and the timing of the heart sounds. It’s especially useful for seeing why S1 (“lub”) coincides with atrioventricular valve closure and S2 (“dub”) with semilunar valve closure. Use it to connect pressure gradients to passive valve opening/closing across diastole, atrial systole, and ventricular systole. Source
the first sound, often written as “lub,” is mainly caused by closure of the atrioventricular valves
the second sound, “dub,” is mainly caused by closure of the semilunar valves
How pressure changes control the cycle
The cardiac cycle is controlled by pressure differences, not by valves opening and closing actively. Valves are passive structures that respond to changes in blood pressure.
This means:
blood flows from higher pressure to lower pressure
valves open when pushed by blood moving forward
valves close when blood begins to push backward
efficient one-way flow depends on correctly timed pressure changes in the chambers
Practical investigation of heart structure and function
The heart can be investigated practically by studying both what it looks like and what it does.
Observing heart structure
A common practical method is a dissection of a mammalian heart, such as a sheep or pig heart. This allows direct observation of structures involved in the cardiac cycle.
Students can identify:
atria and ventricles
thick muscular ventricular walls
atrioventricular and semilunar valves
blood vessels entering and leaving the heart
By gently probing the valves, it is possible to see how their shape supports one-way flow. Comparing the thickness of chamber walls helps link structure to function, especially the need to generate pressure during ventricular systole.
Important precautions include:
wearing gloves and eye protection
using dissecting tools carefully
washing hands and disinfecting surfaces afterward
following teacher instructions for safe disposal of biological material
Investigating heart function
Heart function can be studied in living humans without invasive methods. Common approaches include:
measuring pulse rate at the wrist or neck as an estimate of heart rate
using a heart-rate monitor
listening to heart sounds with a stethoscope
comparing heart rate before and after exercise
These methods help relate observations to the cardiac cycle. For example, a stethoscope allows the valve-closing sounds to be heard, while pulse measurements reflect ventricular contractions sending blood into arteries.
When investigating the effect of exercise on heart activity:
keep the exercise intensity and duration the same for each trial
measure for the same time interval each time
use repeats and calculate a mean
allow a standard rest period before starting
control factors such as body position, temperature, and caffeine intake where possible
This makes the data more valid and reliable.
Improving the quality of data
Pulse investigations can be affected by counting errors, movement, and differences between individuals. To improve quality:
take repeated measurements
use electronic sensors if available
test the same person under different conditions for a fair comparison
record results immediately
look for anomalies rather than ignoring unusual values
Practical investigations are most useful when they connect what is observed, such as pulse or heart sounds, to the sequence of diastole and systole happening inside the heart.
Practice Questions
Explain why the atrioventricular valves close at the start of ventricular systole. (2 marks)
Ventricular pressure rises above atrial pressure. (1)
This prevents backflow of blood into the atria / maintains one-way flow. (1)
Describe what happens during one complete cardiac cycle. Include cardiac diastole, atrial systole, and ventricular systole. (5 marks)
During cardiac diastole, atria and ventricles relax. (1)
Blood enters the atria from veins and the ventricles fill through open atrioventricular valves. (1)
Atrial systole forces the remaining blood into the ventricles. (1)
Ventricular systole raises ventricular pressure and closes the atrioventricular valves. (1)
Semilunar valves open and blood is ejected into the aorta and pulmonary artery; they then close when ventricular pressure falls. (1)
FAQ
The delay allows the atria to finish emptying before the ventricles contract.
This improves ventricular filling and makes the cardiac cycle more efficient. Without this delay, the atria and ventricles could contract too close together, reducing the amount of blood pumped out with each beat.
When heart rate rises, the heart must fit more beats into the same amount of time.
Most of the time saved comes from shortening diastole. This means the ventricles have less time to fill at very high heart rates, which is one reason extremely fast heart rates can reduce pumping efficiency.
Usually, each ventricular contraction produces one pulse in an artery.
However, if a contraction is weak or irregular, it may not create a strong enough pressure wave to be felt at the wrist or neck. In that case, the measured pulse rate can be lower than the actual heart rate.
Valve sounds travel through blood flow and heart tissue, so they are not always heard best directly above the valve itself.
Doctors place the stethoscope at standard listening points where the sound from each valve is transmitted most clearly. This helps them distinguish between normal valve closure sounds and unusual extra sounds or murmurs.
A trained athlete often has a more efficient cardiovascular response.
Their heart can pump a large volume of blood per beat, so it does not need to stay elevated for as long after exercise. Faster recovery also reflects effective control by the autonomic nervous system as the body returns to resting conditions.

.svg){kind=link}
{kind=link}