
Edexcel Syllabus focus:
'Understand the events leading to atherosclerosis, including endothelial dysfunction, inflammatory response, plaque formation and raised blood pressure.'
Atherosclerosis develops gradually in artery walls and underlies many cardiovascular problems. Understanding each stage helps explain how damage to the endothelium can progress to dangerous narrowing and increased blood pressure.
Atherosclerosis as a progressive arterial disease
Atherosclerosis is not a single event. It is a slow, cumulative process that begins with damage or dysfunction in the inner lining of an artery and then develops over time.
Atherosclerosis: A chronic condition in which artery walls become damaged and narrowed by the buildup of fatty plaques.
It mainly affects arteries, where blood travels under high pressure. Because arteries carry blood at high pressure, their walls experience substantial mechanical stress, so small defects in the lining can have major long-term effects.
The key stages required by the specification are linked in sequence:
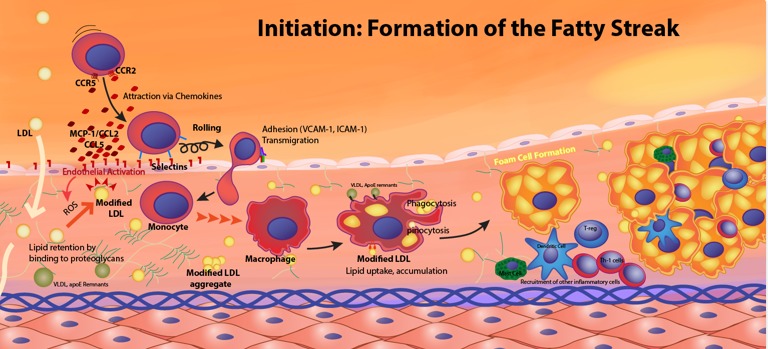
Initiation of atherosclerosis: dysfunctional endothelium promotes adhesion molecule expression (e.g., selectins/VCAM-1), attracting monocytes that migrate into the intima. Monocytes differentiate into macrophages and ingest modified lipoproteins, forming lipid-laden foam cells that drive the early fatty streak. Source
endothelial dysfunction
inflammatory response
plaque formation
raised blood pressure
These events do not happen independently. Each stage makes the next more likely, so atherosclerosis tends to worsen once it has started.
Endothelial dysfunction
The endothelium is the thin layer of cells lining the inside of blood vessels. In a healthy artery, it provides a smooth surface for blood flow and helps maintain normal vessel function.
Endothelial dysfunction: Loss of the normal structure or function of the endothelial lining, making the artery wall more prone to damage and disease.
When endothelial cells become damaged or stop functioning properly, the lining is no longer fully protective. This is the first major step in the development of atherosclerosis.
What changes when the endothelium is dysfunctional?
The lining becomes more permeable, so lipids such as cholesterol-containing particles can move into the artery wall more easily.
The inner surface becomes less smooth, increasing irritation to the vessel wall.
The damaged region can send chemical signals that attract white blood cells.
The artery is less able to maintain normal conditions in the wall, which promotes further injury.
This means endothelial dysfunction does more than simply damage the surface. It creates conditions inside the artery wall that encourage inflammation and the accumulation of material.
Inflammatory response
Once the endothelium is damaged, the body responds as if the artery wall has been injured. This triggers an inflammatory response.
Inflammation is normally protective, but in atherosclerosis it becomes long-term and harmful. White blood cells, especially monocytes, move from the blood into the wall of the artery. These cells develop into macrophages, which take up lipids from the tissue.
As macrophages absorb increasing amounts of lipid, they become swollen and can form foam cells. These cells collect within the artery wall and contribute to an early visible lesion sometimes called a fatty streak. At this point, the artery is already changing structurally.
The inflammatory response also causes more signaling molecules to be released. This attracts additional cells and keeps the process going. Instead of the artery healing completely, the wall remains in a state of chronic inflammation. This is why atherosclerosis is progressive rather than a short-lived response to injury.
Plaque formation
Over time, the lipid deposits, foam cells, and other cellular material build up beneath the endothelium. This produces a plaque or atheroma within the artery wall.
Plaques are not made of fat alone.
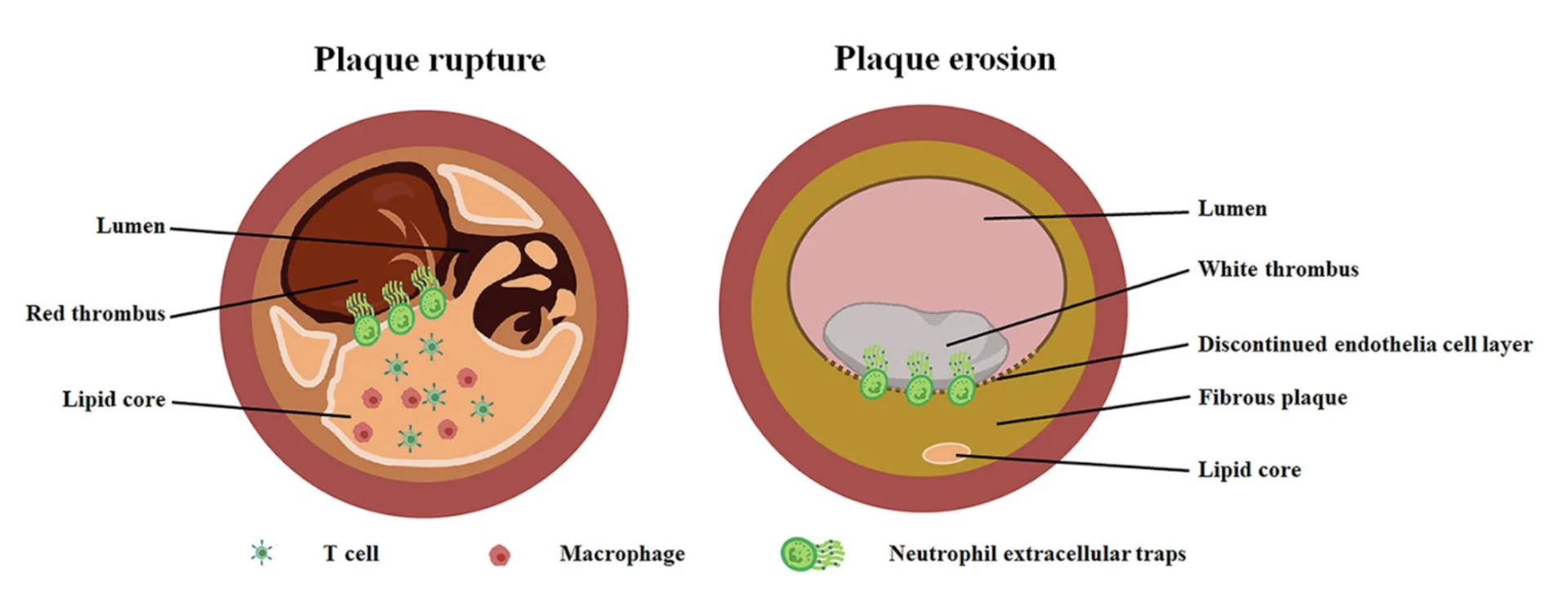
Diagram contrasting plaque rupture and plaque erosion, highlighting major plaque components such as the fibrous cap, lipid core, inflammatory cell-rich regions, and the remaining lumen. It helps link plaque composition and structure to functional consequences like obstruction and endothelial surface disruption. Source
They can contain:
lipids
foam cells and other white blood cells
smooth muscle cells
fibrous tissue, especially collagen
sometimes calcium deposits in more advanced lesions
As the plaque grows, it protrudes into the lumen and reduces the internal diameter of the vessel.
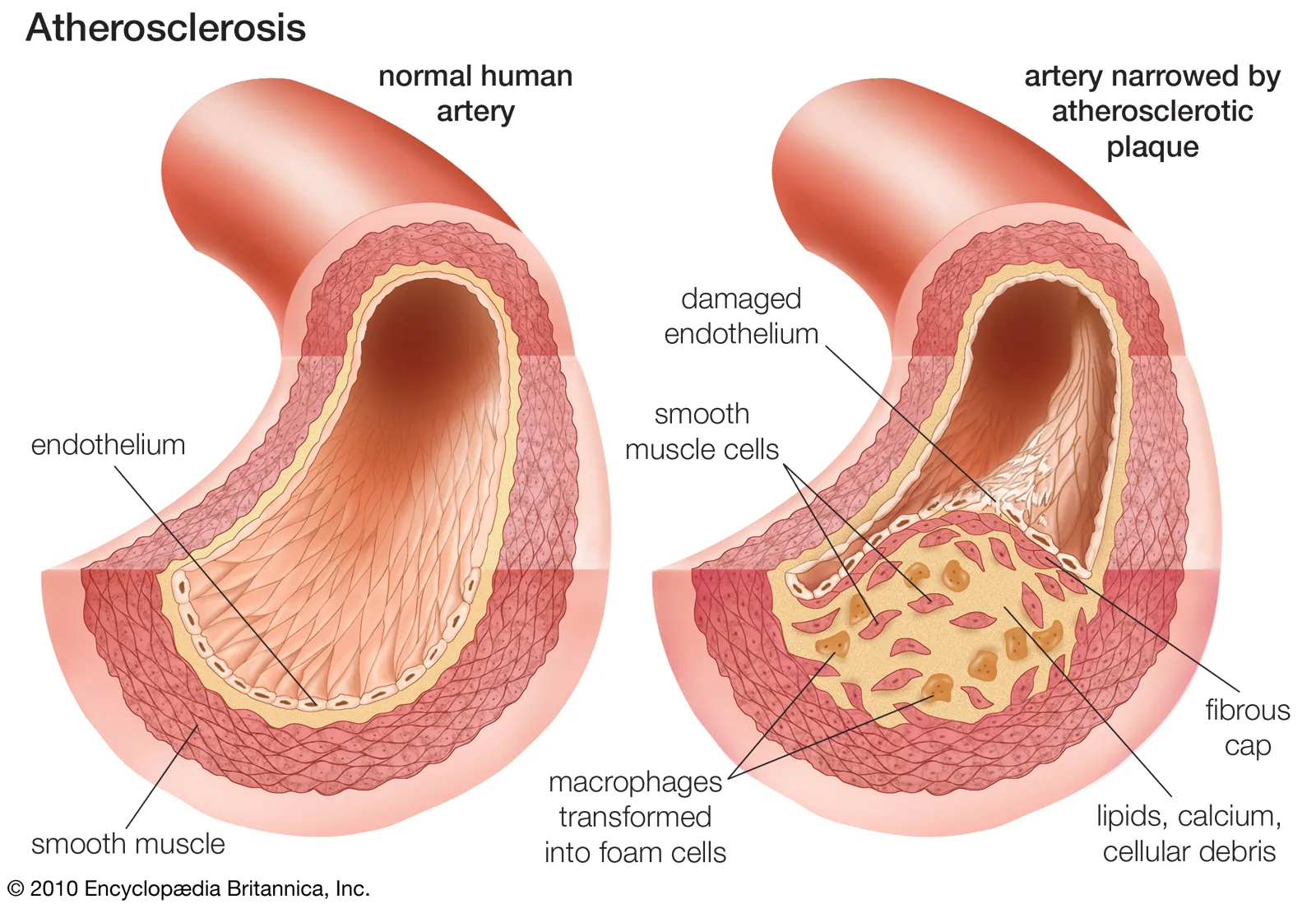
Cross-sectional comparison of a healthy artery versus an atherosclerotic artery showing plaque buildup in the arterial wall and narrowing of the lumen. This structural narrowing increases resistance to flow, helping explain why higher pressure is required to maintain blood flow through affected vessels. Source
The narrowing may be gradual, so the effects often build up over years rather than days.
Why plaque formation is harmful
The artery wall becomes thicker
The lumen becomes narrower
Blood flow becomes less efficient
The wall becomes less elastic
This is especially important in arteries because they must stretch and recoil to help maintain smooth blood flow under pressure. A plaque makes the wall stiffer and less able to respond normally.
How atherosclerosis leads to raised blood pressure
As plaque enlarges, blood has less space to pass through. This increases resistance to blood flow. To push blood through a narrowed artery, a greater pressure is needed.
Raised blood pressure develops for two main reasons:
narrowing of the lumen, which increases resistance
loss of elasticity in the artery wall, which reduces its ability to expand and absorb pressure
When arteries are stiff, they cannot stretch as effectively during ventricular contraction. As a result, pressure in the arterial system increases. The heart must work against a greater load to maintain blood flow through affected vessels.
This raised pressure puts more stress on the vessel wall and can further damage the endothelium. Atherosclerosis can therefore create a vicious cycle:
endothelial dysfunction starts the process
inflammation and plaque formation narrow and stiffen the artery
blood pressure rises
higher pressure causes additional endothelial damage
This positive feedback helps explain why atherosclerosis often worsens over time if the underlying causes are not removed.
Sequence you should know
For Edexcel A-Level Biology, the essential chain of events is:
endothelial dysfunction damages the artery lining
the damage triggers an inflammatory response
lipids and cells accumulate, causing plaque formation
the plaque narrows the lumen and stiffens the wall
this increases resistance and leads to raised blood pressure
Practice Questions
State two ways in which endothelial dysfunction contributes to the development of atherosclerosis. (2 marks)
Endothelium becomes more permeable, allowing lipids or cholesterol-containing particles to enter the artery wall. (1)
Damaged endothelium attracts white blood cells or initiates an inflammatory response. (1)
Explain how atherosclerosis develops from endothelial dysfunction to raised blood pressure. (5 marks)
Any five from:
endothelial lining becomes damaged or dysfunctional
lipids enter and accumulate in the artery wall
inflammatory response occurs
monocytes enter the wall and become macrophages
macrophages take up lipid and form foam cells
plaque or atheroma forms beneath the endothelium
plaque narrows the lumen of the artery
artery wall becomes less elastic or stiffer
increased resistance to blood flow leads to raised blood pressure
FAQ
Blood flow is less smooth at branches and bends than in straight sections of an artery. This creates disturbed flow and uneven mechanical forces on endothelial cells.
Over long periods, these conditions can make the endothelium more vulnerable to dysfunction. That is why plaque formation is often concentrated at specific sites rather than spread evenly along the whole artery.
A fatty streak is an early lesion made mainly of lipid-filled foam cells within the artery wall. It may cause little or no narrowing at first.
A mature plaque is more complex. It usually contains a larger lipid core, more fibrous tissue, and sometimes calcium. Mature plaques are more likely to narrow the lumen and stiffen the artery.
Veins carry blood at much lower pressure than arteries, so their walls experience less mechanical stress. Their endothelial lining is therefore less exposed to the conditions that favor atherosclerotic change.
This difference shows that pressure and flow patterns matter. Atherosclerosis is mainly a disease of arteries because the arterial environment places greater strain on the vessel wall.
Very early changes can sometimes improve if endothelial function recovers and lipid entry into the artery wall is reduced. Early lesions are generally more reversible than advanced ones.
Large, fibrous, or calcified plaques are much harder to remove completely. Even when full reversal does not occur, slowing progression is still biologically important because it reduces further damage to the artery.
The danger of a plaque is not based only on its size. Its composition and location also matter.
Plaques with a large lipid-rich core, a thinner fibrous covering, or more inflammation may be less stable. A plaque in a critical artery can also have greater effects than a similar plaque elsewhere, even if the narrowing is not the most severe.

{kind=link}