
IB Syllabus focus: 'Internal and external validity, extraneous variables, placebos, double-blind procedures and wait-list controls shape causal claims.'
Causal research in psychology asks whether one variable produces change in another. Strong causal claims depend on careful control of threats to validity and on research designs that separate real effects from alternative explanations.
Validity and causal inference
When psychologists investigate cause and effect, they must show that the independent variable produced the observed change in the dependent variable, rather than some uncontrolled influence. Two central ideas are internal validity and external validity.
Internal validity: The extent to which changes in the dependent variable can confidently be attributed to the independent variable rather than other factors.
High internal validity makes a causal conclusion more convincing. If internal validity is weak, a study may still find a difference between groups, but researchers cannot be sure what actually caused it. Even a statistically significant result is not enough if an uncontrolled variable could also explain the findings.
Internal validity and extraneous variables
A major threat to internal validity is the extraneous variable.
Extraneous variable: Any variable other than the independent variable that may affect the dependent variable.
Extraneous variables threaten internal validity because they provide alternative explanations for the results. If an extraneous variable changes systematically with the independent variable, it becomes a confounding variable, and the causal interpretation is much weaker.
Common sources of extraneous variables include:
Participant differences, such as age, motivation, mood, or prior experience
Situational differences, such as noise, room temperature, time of day, or researcher behavior
Procedural inconsistencies, such as different instructions or testing conditions
Changes over time, such as fatigue, practice, boredom, or natural recovery
Researchers try to control these influences by standardizing procedures, randomly allocating participants to conditions, and keeping everything except the independent variable as similar as possible. The better this control, the stronger the causal claim.
External validity
Causal research also needs findings that can be generalized beyond the study itself.
External validity: The extent to which findings can be generalized to other people, settings, situations, or times.
A study may establish cause and effect under controlled conditions but still have limited external validity. This happens when findings do not generalize well to different populations or real-world contexts. Sampling matters here: results from a narrow volunteer sample may not transfer easily to broader groups.
A tightly controlled laboratory experiment can produce strong internal validity, yet the artificial setting may reduce how well the findings reflect everyday behavior. Psychologists therefore balance control with realism when evaluating causal research.
Placebos and expectation effects
One important control in intervention research is the placebo.
Placebo: An inactive treatment or condition that appears real to participants and is used as a comparison in order to control expectation effects.
A placebo condition is useful when participants may improve simply because they expect help.
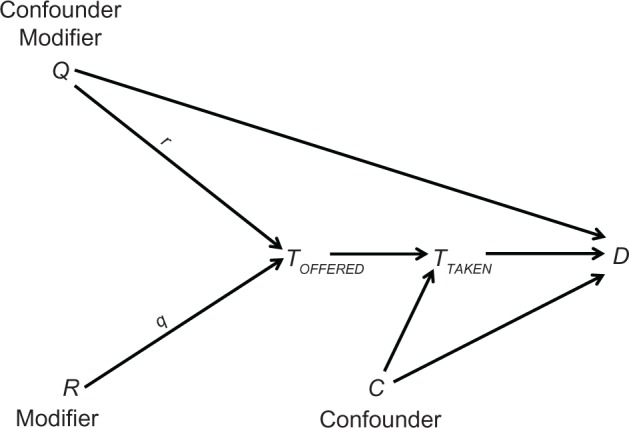
Causal diagram(s) illustrating how treatment assignment, expectations, and outcomes can be linked—and how blinding aims to block biasing pathways. The figure helps students see placebo/expectancy effects as alternative causal routes that can mimic a treatment effect. This visual supports clearer reasoning about which links a study design is trying to control. Source
Comparing a treatment group with a placebo group helps separate the true effect of the independent variable from the effects of expectation, attention, and hope. This strengthens internal validity because improvement cannot automatically be attributed to belief in treatment.
Researchers often combine placebo controls with double-blind procedures.
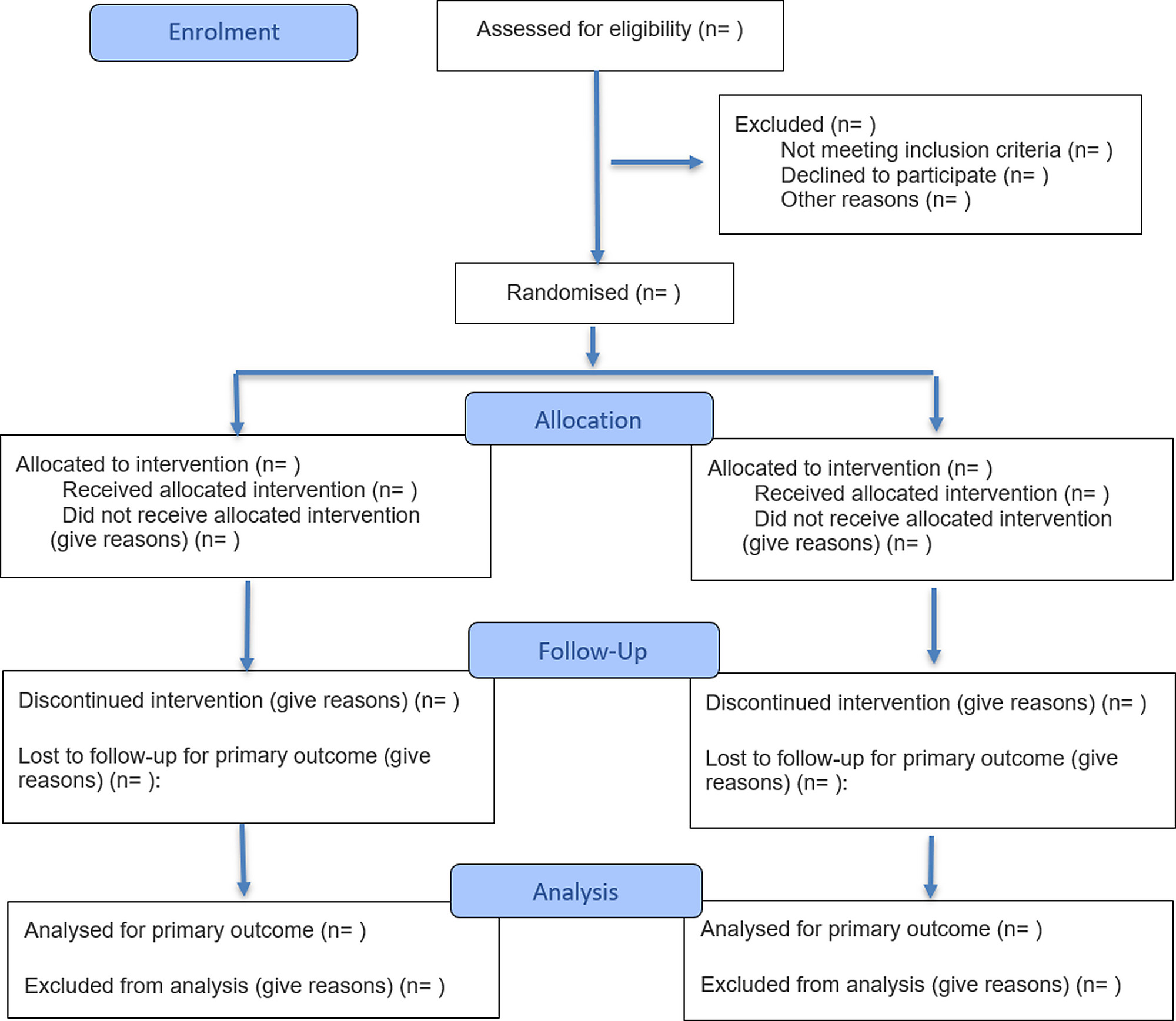
A CONSORT-style participant flow diagram for a randomized trial. It visually tracks enrollment, random allocation to conditions (e.g., treatment vs placebo), follow-up (including dropouts), and analysis. This helps evaluate internal validity by making exclusions and attrition—and their potential to bias results—transparent. Source
Double-blind procedure: A research procedure in which neither the participant nor the researcher who interacts with or assesses the participant knows which condition the participant is in.
Double-blind studies reduce expectancy effects, demand characteristics, and subtle cueing. If participants know they received the real treatment, they may behave differently. If researchers know the condition, they may unintentionally influence participants or interpret ambiguous responses in a way that supports the hypothesis.
Double-blind procedures are especially valuable when outcomes involve judgment, such as symptom ratings or behavioral observations. In some psychological interventions, full blinding is difficult, but when blinding is impossible, causal claims should be evaluated more cautiously.
Wait-list controls
Another useful comparison group is the wait-list control, especially in treatment research.
Wait-list control: A control group that does not receive the treatment during the first phase of a study but is promised the treatment later.
A wait-list control group allows researchers to compare participants who receive treatment immediately with similar participants who have not yet received it. This can strengthen causal inference because differences between groups during the waiting period are more likely to be linked to the treatment itself.
Wait-list controls are common when it would be ethically difficult to withhold a potentially helpful intervention completely. They are often used in therapy, stress-management, or school-based programs where delayed access is acceptable. However, they do not control for placebo effects as well as a matched placebo condition, because participants know they are still waiting for treatment.
Evaluating causal claims
When reading a study, ask whether the design rules out alternative explanations and whether the findings can reasonably generalize beyond the study itself. Strong causal claims usually depend on:
high internal validity through control of extraneous variables
appropriate comparison groups, such as placebo or wait-list controls
blinding procedures that reduce expectancy effects
sufficient external validity to support generalization
In IB answers, link each control directly to the alternative explanation it reduces, and then comment on whether the findings can generalize beyond the study sample and setting.
Practice Questions
Define internal validity. [2 marks]
1 mark for identifying internal validity as the extent to which a study supports a cause-and-effect conclusion.
1 mark for stating that changes in the dependent variable must be attributable to the independent variable rather than extraneous variables or other factors.
Explain how placebos, double-blind procedures, and wait-list controls can strengthen causal claims in psychological research. [6 marks]
Up to 2 marks for explaining that a placebo controls for expectation effects, so improvement cannot automatically be attributed to belief or attention alone.
Up to 2 marks for explaining that a double-blind procedure reduces participant and researcher expectancy effects, cueing, or biased assessment.
Up to 1 mark for explaining that a wait-list control provides a comparison group that has not yet received treatment, helping isolate treatment effects.
Up to 1 mark for clearly linking these controls to stronger internal validity and therefore stronger causal inference.
FAQ
An active control group is often better when a placebo would be too obvious or unrealistic.
For example, if a treatment involves therapist contact, training, or noticeable side effects, an active control can match time, attention, and structure more closely than a placebo. This helps researchers test whether the specific treatment works better than a credible alternative, not just better than doing almost nothing.
Unblinding happens when participants or researchers correctly guess which condition someone is in.
Once that happens, expectations can return and influence self-report, effort, observer ratings, or behavior. Researchers sometimes test the success of blinding afterward by asking people to guess their condition. If guesses are much better than chance, the protection offered by the double-blind design is reduced.
Attrition means participants drop out before the study ends.
If more people leave the wait-list group than the treatment group, the groups may no longer be comparable. That can distort the apparent treatment effect, because differences at the end may reflect who stayed in the study rather than the treatment itself. Researchers try to reduce this problem with good follow-up procedures and careful data analysis.
Therapist effects occur when outcomes depend partly on who delivers the treatment, not just on the treatment itself.
A highly skilled, warm, or enthusiastic therapist may produce better outcomes than another therapist using the same method. Researchers may reduce this threat by using treatment manuals, training therapists similarly, and checking treatment fidelity. Without this control, it is harder to know whether the intervention caused the improvement.
Efficacy asks whether a treatment works under highly controlled conditions.
Effectiveness asks whether it works in everyday settings, with typical clients, staff, and practical constraints. A study can show strong efficacy but still have limited effectiveness if real-world conditions differ too much from the research setting. This distinction is useful when deciding how far causal findings should be generalized.
