
IB Syllabus focus: 'Gender and cultural biases can affect clinical diagnosis, prevalence statistics and treatment decisions.'
Clinical psychologists try to identify and treat distress accurately, but ideas about “normal” behavior are shaped by gender expectations and cultural norms, creating bias in diagnosis, reported prevalence, and treatment planning.
Why this issue matters
Clinical psychology depends on judgment.
A clinician must decide whether a behavior is a symptom, how severe it is, and which treatment is most appropriate. These decisions are influenced by diagnostic manuals, interview methods, and professional training, but they can also be influenced by social assumptions.
One important risk is gender bias.
Gender bias: A systematic distortion in judgment or practice caused by assumptions about gender, leading clinicians to interpret symptoms, risk, or behavior differently for different genders.
Gender bias may appear when clinicians expect certain disorders to be “male” or “female.” This can affect what questions they ask, which symptoms they notice, and how seriously they take reported distress. For example, a clinician may be more likely to recognize anxiety in women because it fits a stereotype, while missing it in men if it appears as irritability, anger, or substance misuse.
Another important risk is cultural bias.
Cultural bias: A distortion in assessment or treatment that occurs when the values, norms, or expectations of one cultural group are treated as universal.
Cultural bias happens when clinicians judge a person’s behavior against standards drawn mainly from a dominant culture. Patterns of eye contact, emotional expression, family dependence, spiritual beliefs, and ways of describing distress differ across cultures. If these differences are misunderstood, normal or culturally meaningful behavior may be labeled as abnormal.
Gender bias in diagnosis
Gender bias can affect diagnosis in several ways:
Stereotyped symptom expectations: Clinicians may expect women to show internalizing symptoms such as sadness or worry, and men to show externalizing symptoms such as aggression. This can hide symptoms that do not match those expectations.
Different thresholds for concern: The same behavior may be judged differently depending on the client’s gender. Emotional intensity in women may be pathologized more quickly, while risk-taking in men may be normalized.
Underdiagnosis and overdiagnosis: Some disorders may be underrecognized in one gender and overrecognized in another because diagnostic criteria were developed from unbalanced samples or because clinicians rely on stereotypes.
This matters because diagnosis is not just a label. It shapes access to support, insurance coverage, treatment plans, and how a client understands their own difficulties.
Cultural bias in diagnosis
Cultural bias in diagnosis often begins with the question: whose norms define mental health? If diagnostic standards are based mostly on Western, urban, individualist assumptions, then people from different cultural backgrounds may be judged unfairly.
Common sources of cultural bias include:
Language differences: A client may describe distress through physical symptoms, metaphors, or spiritual language that a clinician misreads.
Communication style: Limited eye contact, silence, indirect speech, or emotional restraint may reflect respect or cultural convention rather than pathology.
Different meanings of symptoms: Hearing the voice of an ancestor, strong religious experiences, or collective family decision-making may be culturally meaningful rather than signs of disorder.
Mistrust of services: Clients from marginalized groups may appear guarded or suspicious because of previous discrimination, not because of psychosis or paranoia.
Cultural bias is especially likely when clinicians fail to ask what the symptom means to the client and their community.
Bias and prevalence statistics
Prevalence statistics describe how common a disorder appears to be in a population.
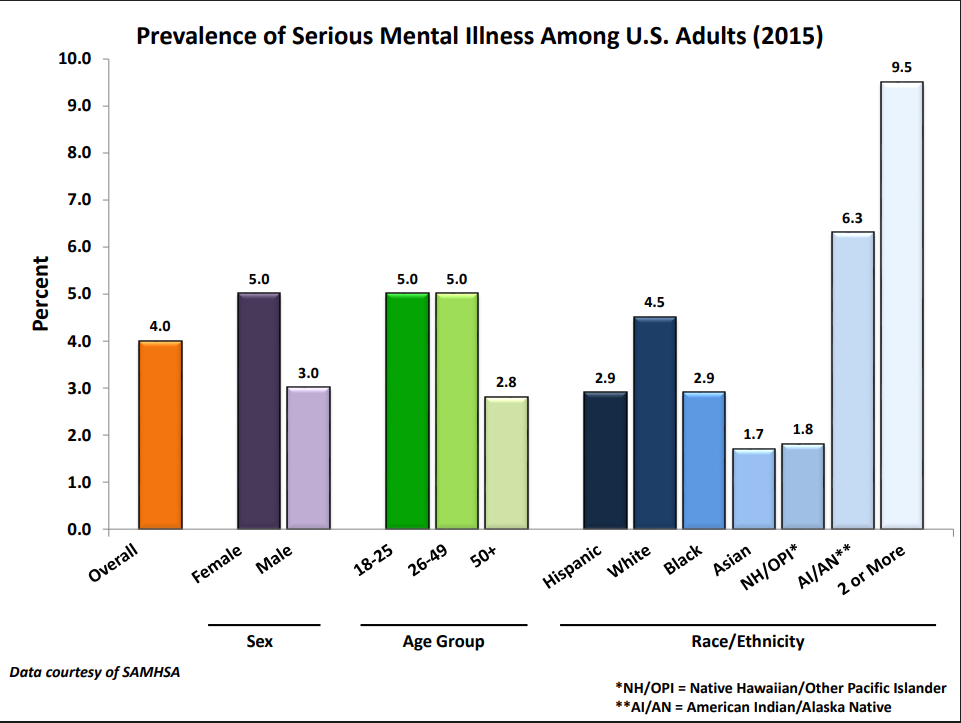
This NIMH/SAMHSA bar chart visualizes differences in the estimated prevalence of serious mental illness across demographic groups (including sex and race/ethnicity). It helps illustrate why prevalence data can look uneven across groups, and why interpretation should consider help-seeking, access to services, and potential diagnostic/measurement bias. Source
However, prevalence is affected not only by actual rates of disorder, but also by who gets diagnosed and counted.
Gender and cultural bias can distort prevalence statistics through:
Help-seeking differences: Some groups are less likely to seek treatment because of stigma, cost, or distrust.
Access to services: If one group has better access to mental health care, that group may appear to have higher prevalence simply because more cases are identified.
Diagnostic bias: If clinicians are more likely to diagnose a disorder in one gender or cultural group, prevalence figures may exaggerate group differences.
Measurement tools: Questionnaires and interviews may fit one population better than another, producing unequal detection rates.
As a result, prevalence data should not be treated as a perfect reflection of “true” disorder rates. They may also reflect the biases built into systems of assessment.
Bias and treatment decisions
Bias continues after diagnosis. Treatment decisions can also be shaped by gendered and cultural assumptions.
Examples include:
assuming one gender is more compliant, resilient, or emotionally expressive than another
preferring medication over psychotherapy, or vice versa, based on stereotypes rather than client needs
overlooking the role of family, religion, migration, discrimination, or community support in the client’s recovery
choosing treatments based on Western values of independence and verbal self-disclosure even when these do not fit the client’s background
A treatment that ignores culture may be less effective because it feels irrelevant, disrespectful, or unsafe. Likewise, treatment influenced by gender stereotypes may fail to address the client’s real concerns.
Reducing bias in clinical psychology
Clinicians cannot remove all bias completely, but they can reduce it through careful practice.
Useful strategies include:
reflecting on personal assumptions about gender, normality, and distress
using assessment tools validated for diverse populations
asking open questions about the meaning of symptoms in the client’s cultural context
gathering information from multiple sources rather than relying on first impressions
considering how discrimination, social roles, and power differences affect mental health
adapting treatment plans to the client’s language, values, and support systems
Good clinical practice requires more than technical skill. It also requires awareness that diagnosis, prevalence, and treatment are shaped by social context as well as symptoms.
Practice Questions
State one way cultural bias can affect clinical diagnosis. [2 marks]
1 mark for identifying a relevant effect, such as judging behavior by the norms of a dominant culture.
1 mark for linking that effect to diagnosis, for example mislabeling culturally normal behavior as abnormal.
Explain how gender bias and cultural bias may influence prevalence statistics and treatment decisions in clinical psychology. [6 marks]
1–2 marks for explaining gender bias, such as stereotypes affecting who is diagnosed or what treatment is offered.
1–2 marks for explaining cultural bias, such as using one culture’s norms as universal in assessment or treatment.
1 mark for linking bias to prevalence statistics, for example distorted rates due to unequal diagnosis, help-seeking, or access.
1 mark for linking bias to treatment decisions, for example inappropriate therapy choices or poor cultural fit.
Full marks require clear psychological terminology and applied explanation rather than simple description.
FAQ
Translation does not guarantee that a measure means the same thing in two cultures.
Problems can include:
different meanings for emotion words
culture-specific idioms of distress
response styles, such as avoiding extreme answers
items that assume Western lifestyles or family structures
A questionnaire may be linguistically correct but still lack conceptual equivalence, meaning it does not measure the same psychological experience across groups.
A cultural formulation interview is a structured way of asking how clients understand their problem within their own social and cultural world.
It can help clinicians explore:
the client’s explanation for symptoms
stressors and supports
cultural identity
barriers to care
preferences for help
This reduces the chance of making quick assumptions based only on diagnostic checklists.
Not automatically.
A shared background may improve trust, communication, and cultural understanding, but bias can still occur. People from the same group do not all share the same beliefs, values, or experiences.
Good practice depends more on:
listening carefully
avoiding stereotypes
checking assumptions
adapting treatment collaboratively
Matching can help, but it is not a complete solution.
Many clinical systems were designed around binary assumptions about gender.
This can create problems such as:
intake forms that force inaccurate categories
clinicians misreading gender-related stress as disorder
confusion between identity and pathology
treatment plans that ignore minority stress, discrimination, or safety concerns
Bias may be reduced when clinicians use affirming language, ask rather than assume, and separate identity from symptoms.
When criteria are revised, prevalence can rise or fall even if the underlying level of distress stays similar.
This may happen because:
thresholds become broader or narrower
examples better fit some groups than others
new guidance changes how clinicians interpret symptoms
cultural notes reduce some kinds of misdiagnosis
So long-term prevalence comparisons should be made carefully, especially when manuals or criteria have changed.
