
AP Syllabus focus:
‘Color vision deficiency can result from problems with cones or ganglion cells, and damage to visual brain areas can produce prosopagnosia or blindsight.’
Visual problems can arise when the eye’s receptors miscode light or when the brain’s visual pathways fail to interpret normal input. This page focuses on colour vision deficiency and two brain-based disorders: prosopagnosia and blindsight.
Visual disorders vs. brain-based vision problems
Where vision can break down
Retinal/receptor-level disruption: the sensory hardware is altered (e.g., cone dysfunction), changing the raw signal sent onward.
Post-retinal/brain-level disruption: eyes may be intact, but visual cortex or associated networks cannot interpret the signal normally.
A practical AP distinction: receptor problems often affect what is detected (e.g., colour), while cortical problems often affect meaning (e.g., recognising a face).
Colour vision deficiency (cones and ganglion cells)
What “colour vision deficiency” means
Colour perception depends on cone photoreceptors and downstream coding by retinal ganglion cells that carry signals via the optic nerve.
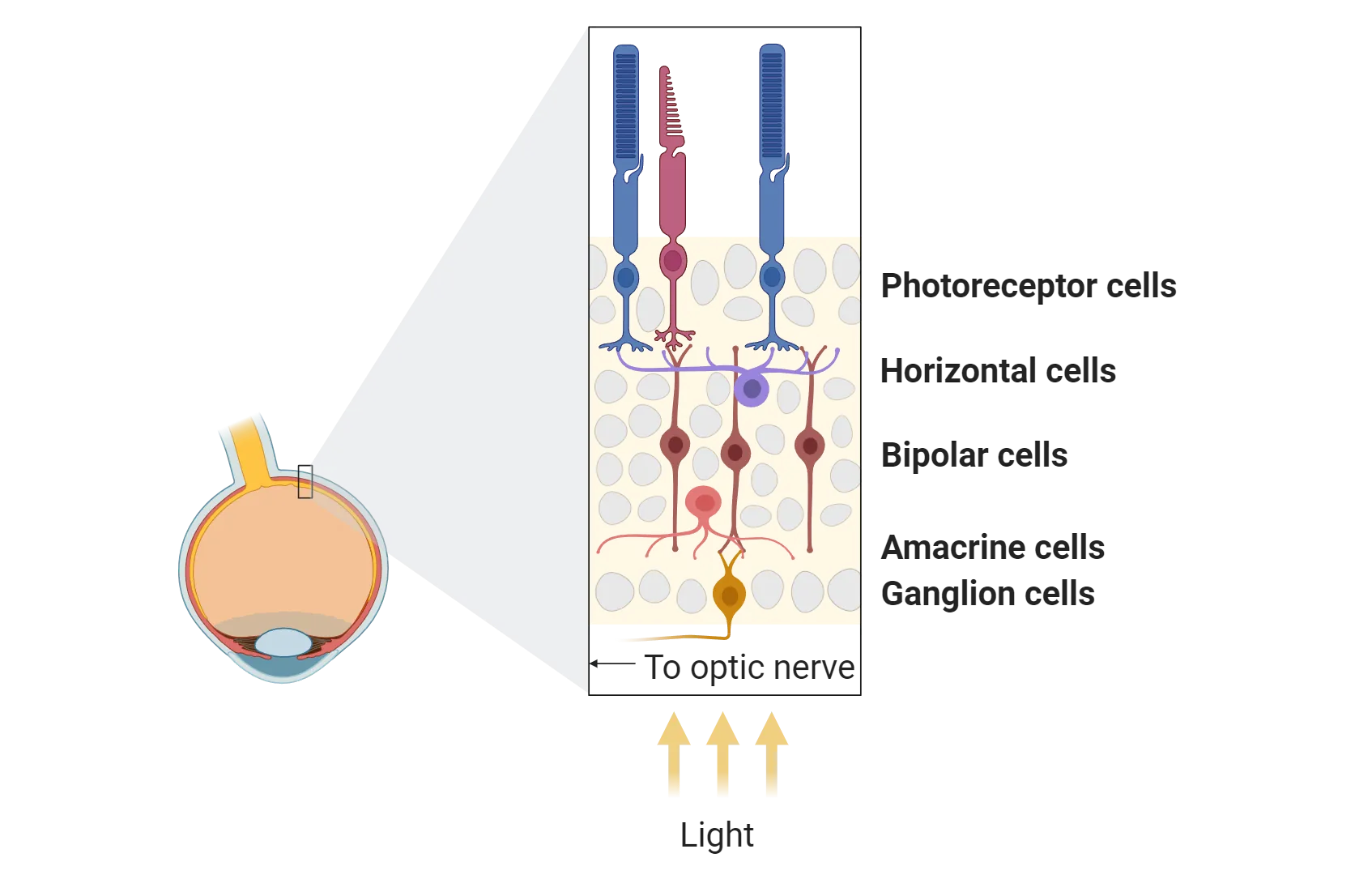
This diagram summarizes the retina’s layered circuitry, highlighting how signals flow from photoreceptors (rods/cones) to bipolar cells and then to retinal ganglion cells whose axons form the optic nerve. It helps explain why color-vision problems can arise either from altered cone photopigments (input stage) or from atypical ganglion-cell coding (output stage). Source
Disruption at either level can produce atypical colour experience.
Colour vision deficiency: reduced or altered ability to discriminate colours due to atypical functioning of colour-processing mechanisms in the retina (e.g., cones) and/or retinal output pathways (e.g., ganglion cells).
Cones: receptor-level causes
Cones normally respond best to different wavelengths; if a cone type is absent or functions atypically, colour discrimination changes.
Missing/altered cone pigments can reduce sensitivity to certain wavelength ranges.
Effects are often most noticeable when colours must be distinguished without brightness cues (e.g., similarly lit reds vs. greens).
Ganglion cells: output-level causes
Even with working cones, retinal ganglion cells can miscode colour contrasts.
Some ganglion cells contribute to opponent-like signalling (contrast between colour channels).
If these pathways are disrupted, the brain receives a degraded or biased “difference” signal, producing colour confusions that are not fully explained by cone loss alone.
What students should be able to do
Identify cones and ganglion cells as potential loci of colour-vision problems.
Predict that colour-related errors can occur despite otherwise sharp visual acuity.
Brain-based vision problems: when the cortex is damaged
Prosopagnosia (face blindness)
Prosopagnosia reflects impaired face recognition due to damage in visual processing regions important for faces (often in the right temporal-occipital area, including the fusiform face area).
Basic vision can be normal: people may still describe features, but fail to recognise identity.
Prosopagnosia: a brain-based impairment in recognising faces, typically following damage to face-processing regions in the temporal-occipital cortex.
People with prosopagnosia often compensate by using non-face cues:
voice, hairstyle, gait, context, distinctive clothing
deliberate feature-by-feature strategies (less efficient than normal holistic processing)
Blindsight
Blindsight occurs when damage (often to primary visual cortex, V1) eliminates conscious visual experience in part of the visual field, yet the person can still respond to some visual information above chance (e.g., guessing motion direction).
Blindsight: responding to visual stimuli without conscious awareness, typically after damage to primary visual cortex affecting part of the visual field.
A key AP idea is dissociation:
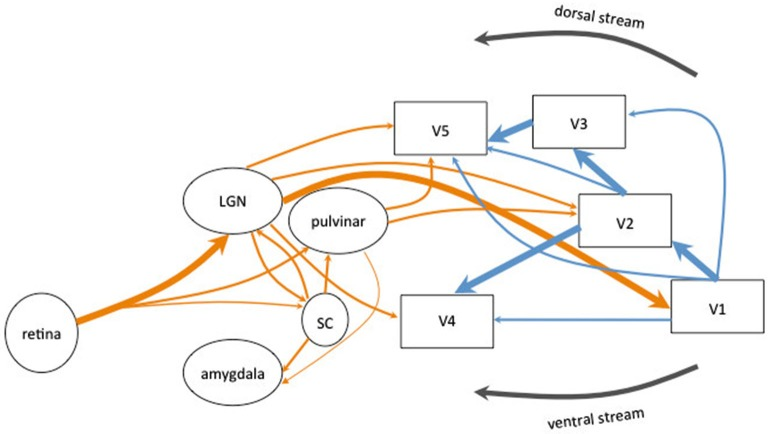
This schematic contrasts the main geniculostriate pathway (retina → LGN → V1) with alternative subcortical routes that can bypass V1 and still drive responses in extrastriate cortex (e.g., via the superior colliculus and pulvinar to MT/V5). It provides an anatomical basis for blindsight: behaviorally relevant visual processing can persist even when conscious visual experience is disrupted by V1 damage. Source
Conscious awareness of seeing can be absent,
while nonconscious processing can still guide behaviour via alternative pathways (e.g., midbrain routes such as the superior colliculus to other cortical areas).
How brain-based problems differ from eye-based problems
Eye-based deficits typically reduce the quality of incoming signals for everyone downstream.
Cortex-based deficits can be selective (e.g., faces) and can spare detection while impairing recognition, or spare performance while removing awareness (blindsight).
Practice Questions
Explain how colour vision deficiency may result from problems with cones or ganglion cells. (1–3 marks)
1 mark: Mentions cones as receptors involved in colour coding and that cone problems can impair colour discrimination.
1 mark: Mentions ganglion cells as retinal output cells involved in transmitting/processing colour information.
1 mark: Explains that disruption at either level can lead to colour confusions/atypical colour perception.
Describe prosopagnosia and blindsight as brain-based vision problems and explain how each illustrates that normal visual input and conscious visual experience can be dissociated. (4–6 marks)
1 mark: Defines/accurately describes prosopagnosia as impaired face recognition due to brain damage.
1 mark: Links prosopagnosia to damage in face-processing areas (e.g., fusiform/temporal-occipital cortex).
1 mark: Notes that basic vision can be intact but recognition/meaning is impaired.
1 mark: Defines/accurately describes blindsight as responding to visual stimuli without conscious awareness.
1 mark: Links blindsight to damage to primary visual cortex () affecting part of the visual field.
1 mark: Explains dissociation: some visual processing can guide behaviour without conscious seeing.
FAQ
They embed numbers/patterns in coloured dot fields that rely on red–green (or other) colour contrasts rather than brightness.
If a viewer cannot separate the intended contrast channel, the figure is missed or misread.
Yes. Some cases follow retinal disease, optic nerve damage, or cortical injury affecting colour processing.
Acquired cases may be asymmetric (one eye more affected) and can involve broader colour loss than typical inherited forms.
Face identity relies heavily on specialised visual networks, while voice identity relies on auditory and multimodal networks.
Damage can be relatively selective, leaving non-visual person-recognition routes available.
Beyond the classic retina $\rightarrow$ LGN $\rightarrow V1$ route, signals can travel via subcortical pathways, such as:
retina $\rightarrow$ superior colliculus
superior colliculus $\rightarrow$ pulvinar and extrastriate areas
These routes can support crude detection without normal awareness.
No. Some individuals show developmental prosopagnosia without an obvious lesion.
Research suggests atypical development or connectivity in face-processing networks can produce lifelong face-recognition difficulty.
