
AP Syllabus focus:
‘Pain is processed in body and brain; gate control theory and phantom limb sensation highlight pain complexity, while vestibular and kinesthetic senses support balance and coordinated movement.’
Pain, balance, and body position rely on coordinated signals from receptors, spinal pathways, and brain systems. These processes shape protective responses, movement control, and everyday awareness of where the body is in space.
Pain: from receptors to the brain
Pain is both a sensory experience (where it hurts, how intense) and an affective experience (how unpleasant it feels). It begins with specialized receptors and is constructed through nervous system processing.
Nociception and pain pathways
Nociception: The detection and transmission of potentially tissue-damaging stimuli by sensory receptors and neural pathways.
Key steps and structures:
Nociceptors in skin, muscles, joints, and organs respond to extreme pressure, heat/cold, or chemicals released by inflammation.
Signals travel along afferent sensory fibres to the spinal cord, where interneurons help route information upward.
Ascending pathways project to brain regions involved in:
Somatosensory cortex (location and physical quality of pain)
Thalamus (major relay for sensory information)
Limbic-related circuits (emotional distress and motivational response)
The brain can also send descending signals that increase or reduce pain signalling at the spinal level.
Pain perception varies across people and situations because attention, stress, expectation, and context alter how strongly the brain weights incoming nociceptive input.
Gate control theory (why pain is “modulatable”)
Gate control theory: The idea that the spinal cord contains a neurological “gate” that either blocks pain signals or allows them to pass to the brain, influenced by other sensory input and by brain activity.
In practice, the “gate” can be affected by:
Competing touch/pressure signals (e.g., rubbing an injured area can reduce pain)
Attention and emotion (anxiety can amplify; distraction can dampen)
Brain-based modulation (top-down control can inhibit spinal transmission)
This helps explain why pain is processed in both the body and brain: tissue signals matter, but interpretation and modulation are central to the final experience.
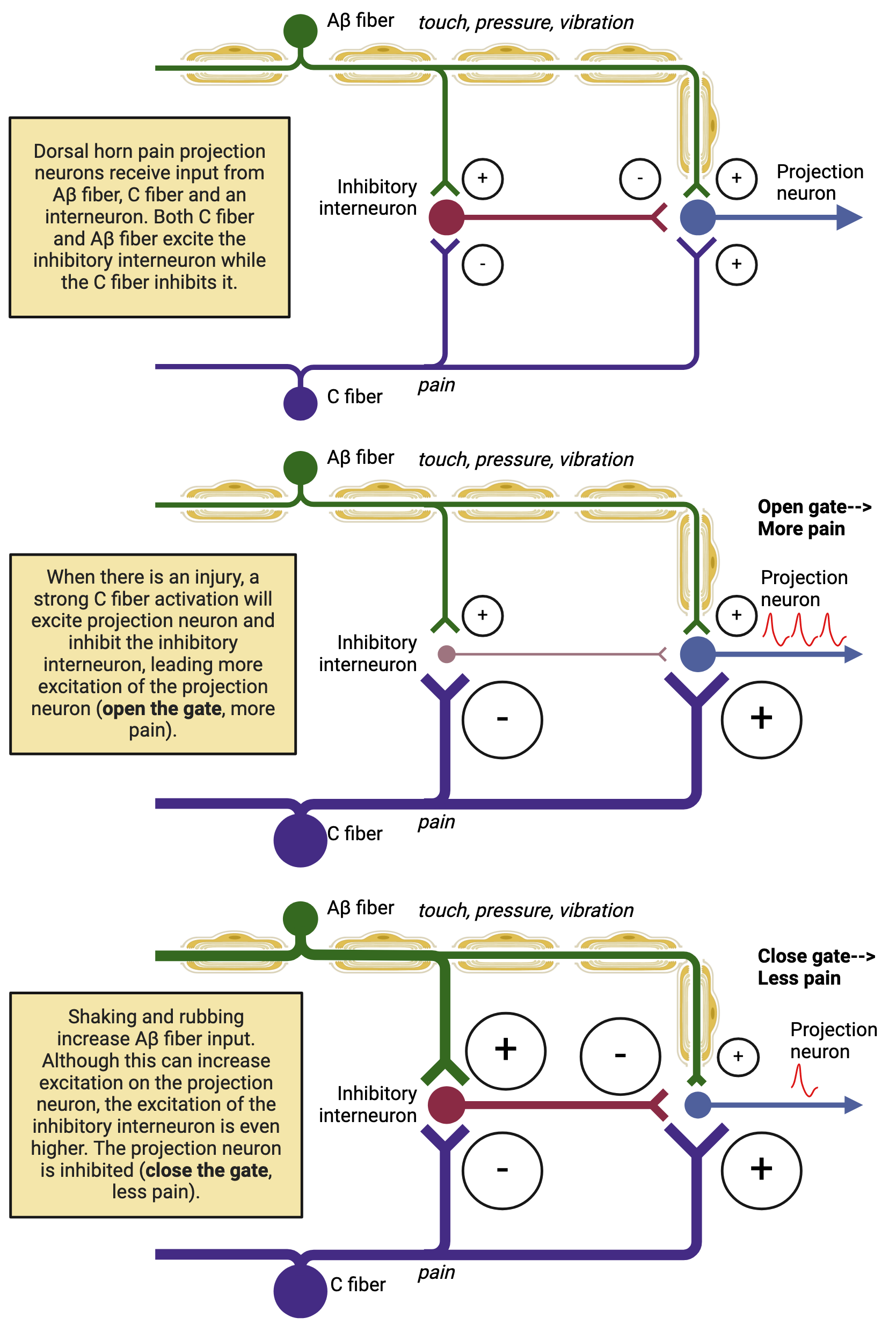
Diagram of gate control theory showing how large-diameter touch input (Aβ fibers) can activate inhibitory interneurons in the spinal cord, reducing firing in the pain projection neuron. In contrast, strong nociceptive input (C fibers) promotes projection-neuron activity, effectively “opening” the gate. This visual reinforces that pain is shaped by spinal-cord circuitry plus top-down modulation—not just tissue damage. Source
Phantom limb sensation (pain without peripheral input)
Phantom limb sensation occurs when someone experiences feelings (including pain) in an amputated or missing limb. It highlights that pain is not merely a direct readout of tissue damage.
The brain areas that previously represented the limb can remain active.
Sensory and motor circuits may continue generating body-related signals (“the limb should be there”).
Reorganization of cortical maps can contribute to unusual referred sensations and persistent discomfort.
Balance: vestibular sense
Balance depends heavily on the vestibular system in the inner ear, which provides continuous information about head movement and orientation relative to gravity.
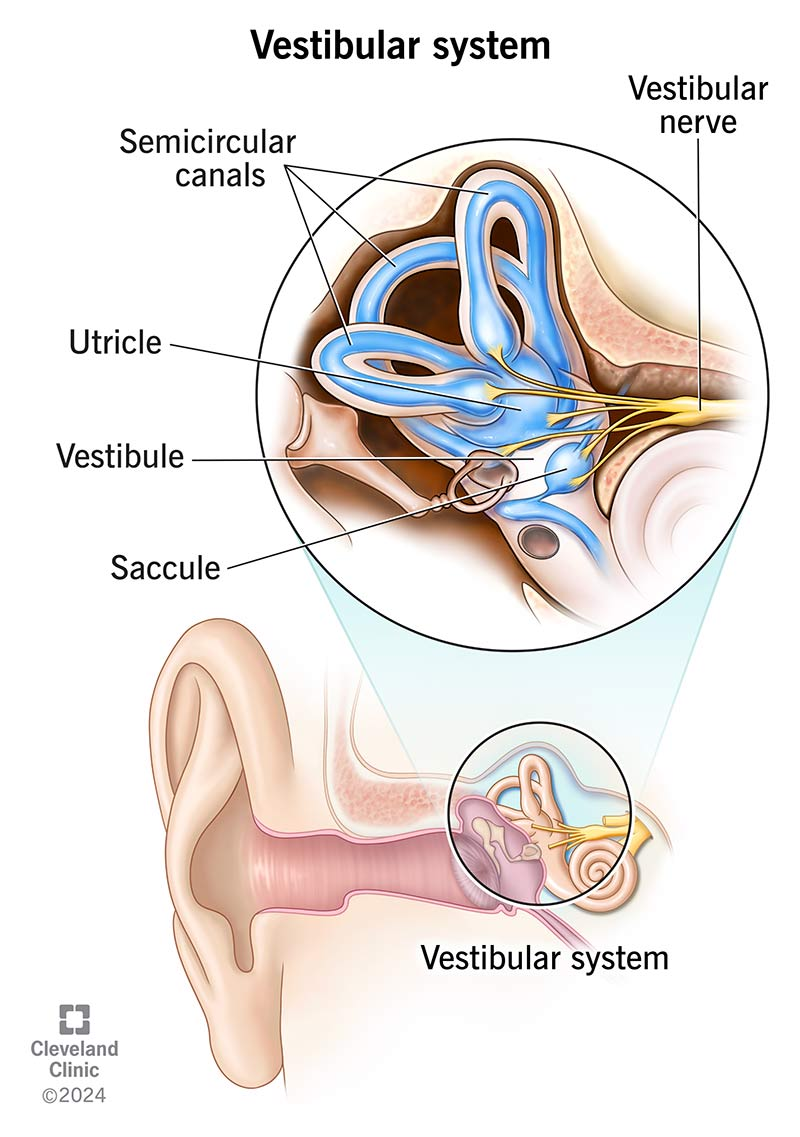
Labeled inner-ear diagram identifying the three semicircular canals and the otolith organs (utricle and saccule) within the vestibule. The figure helps you map structure to function: semicircular canals encode rotational movements, while the otolith organs encode linear acceleration and head tilt relative to gravity. It also shows the vestibular nerve pathway carrying these signals to the brain. Source
How the vestibular system supports equilibrium
Vestibular sense: The system that monitors head position and movement using inner-ear structures, supporting balance, posture, and stabilised vision.
Core components and functions:
Semicircular canals detect rotational head movement.
Otolith organs (vestibular sacs) detect linear acceleration and tilt.
Vestibular signals integrate with:
Vision (to stabilise gaze during movement)
Somatosensory input from muscles and joints (to adjust posture)
Outputs help coordinate:
Postural reflexes (automatic adjustments to prevent falling)
Eye movements that maintain stable visual perception while the head moves
Body position: kinesthetic (proprioceptive) sense
Kinesthesia (often called proprioception) supports coordinated movement by continuously tracking limb position and motion, even with eyes closed.
Kinesthetic inputs and coordinated movement
Kinesthetic sense (proprioception): Feedback from muscles, tendons, and joints that provides information about the position and movement of body parts.
Major information sources include:
Muscle spindles (muscle stretch/length changes)
Golgi tendon organs (tension changes)
Joint receptors (joint angle and movement)
Kinesthetic input supports:
Smooth motor coordination by updating the brain about current body configuration
Rapid corrections during movement (especially when combined with vestibular and visual cues)
Skilled actions that depend on precise timing and position information (e.g., reaching, walking, maintaining stance)
Practice Questions
Explain the gate control theory of pain. (2 marks)
1 mark: States that pain transmission is modulated by a “gate” mechanism in the spinal cord.
1 mark: Explains that the gate can be opened/closed by other sensory input and/or top-down brain influences, altering perceived pain.
Discuss how vestibular and kinesthetic senses contribute to balance and coordinated movement. Include at least one detail about the sensory structures involved. (6 marks)
1 mark: Identifies vestibular sense as supporting balance/equilibrium.
1 mark: Identifies kinesthetic (proprioceptive) sense as providing body position/movement information.
1 mark: Names a vestibular structure (e.g., semicircular canals or otolith organs/vestibular sacs).
1 mark: Describes what that vestibular structure detects (rotation vs linear acceleration/tilt).
1 mark: Names a kinesthetic receptor source (e.g., muscle spindles, Golgi tendon organs, joint receptors).
1 mark: Explains integration for coordinated movement (e.g., posture adjustments, stabilised gaze, motor corrections).
FAQ
Ongoing pain can reflect changes in nervous system processing rather than ongoing tissue damage.
Possible mechanisms include increased spinal excitability, altered brain representation of the painful area, and learned associations that heighten threat responses.
Motion sickness often arises from conflict between sensory signals.
Vestibular system signals movement
Visual system may signal stability (or the opposite)
The mismatch can trigger nausea and dizziness
Yes, partially, through compensation.
Vision and proprioception can be used more heavily, and the brain can recalibrate with practice, though rapid head movements and low-light conditions may remain difficult.
Common methods include joint-position matching tasks and movement-detection tests.
A clinician may move a finger or toe slightly and ask the person to report direction, or ask them to mirror-match limb positions with eyes closed.
Referred pain can occur when sensory neurons from different body regions converge on shared spinal pathways.
The brain may misattribute the source based on typical patterns of activation, leading to pain felt in a different location than the actual origin.
