
AP Syllabus focus:
‘Brain plasticity allows rewiring after damage, and researchers study brain function using scans such as EEG and fMRI, case studies, and lesioning.’
Brain function is not fixed: experience, development, and injury can change neural connections. Psychologists study these changes and link brain activity to behaviour using complementary research methods, each with distinct strengths and limits.
Brain plasticity (rewiring)
Brain plasticity refers to the brain’s capacity to change structurally and functionally in response to experience or damage. Plasticity supports learning and recovery, but it is constrained by biology (age, location of injury, and available neural pathways).
Brain plasticity: the brain’s ability to reorganise by forming, strengthening, weakening, or reassigning neural connections across the lifespan.
How plasticity happens
Synaptic strengthening/weakening: frequently used connections become more efficient; unused connections may weaken.
Cortical remapping: nearby brain regions can sometimes take over functions after injury (often partial rather than complete recovery).
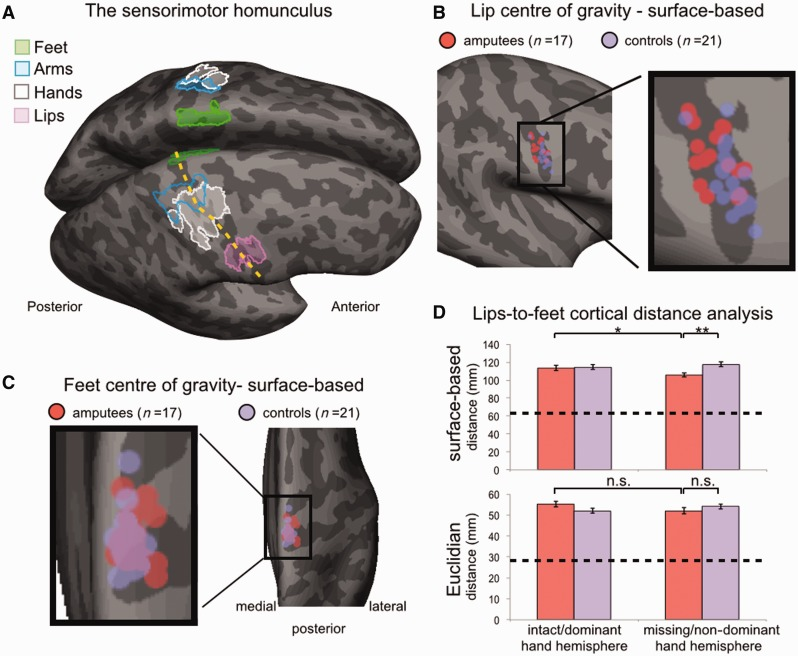
Figure illustrating the human sensorimotor homunculus mapped onto the cortical surface near the central sulcus, with different body-part representations labeled by region. It provides a concrete example of how functions are topographically organized, which is the basis for understanding (often limited) remapping after loss of input or injury. Source
Compensation: people may recruit different neural networks or strategies to achieve similar behavioural outcomes.
Experience-dependent change: practice (e.g., skill learning) can alter network efficiency and connectivity.
Plasticity after damage: key implications
Greatest plasticity in childhood, but meaningful change still occurs in adults.
Rehabilitation matters: targeted practice can encourage adaptive reorganisation; maladaptive plasticity can also occur (e.g., inefficient compensatory habits).
Limits: severe or widespread damage, or loss of specialised tissue, reduces the degree of functional “rewiring.”
Brain research methods: linking brain and behaviour
Researchers choose methods based on whether they need timing, location, causal evidence, or deep description of an individual.
EEG (electrical activity)
EEG (electroencephalogram): a recording of the brain’s electrical activity via electrodes placed on the scalp.
EEG is especially useful for tracking rapid changes in brain activity over milliseconds.
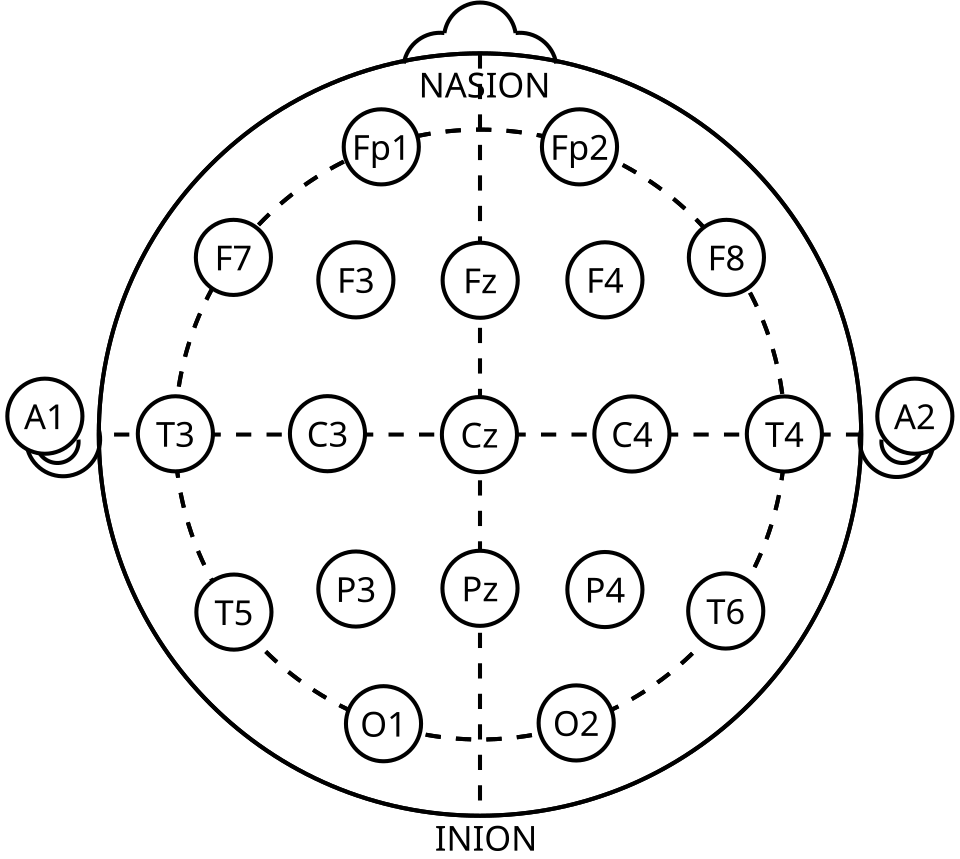
Diagram of the International 10–20 EEG electrode placement system, showing labeled scalp electrode positions (e.g., Fp, F, C, P, O sites and midline “z” electrodes). This reinforces that EEG measures voltage changes at the scalp with excellent timing, but that source localization is inherently indirect. Source
Strengths:
High temporal resolution (precise timing)
Non-invasive; relatively affordable
Limitations:
Low spatial resolution (hard to pinpoint deep or exact sources)
Sensitive to noise (e.g., muscle movement)
A common AP-style interpretation is: EEG is better for when processes occur than where they occur.
fMRI (blood-oxygen changes)
fMRI (functional magnetic resonance imaging): a technique that estimates brain activity by detecting changes in blood oxygenation (the BOLD signal).
fMRI helps identify which brain areas are more active during a task.
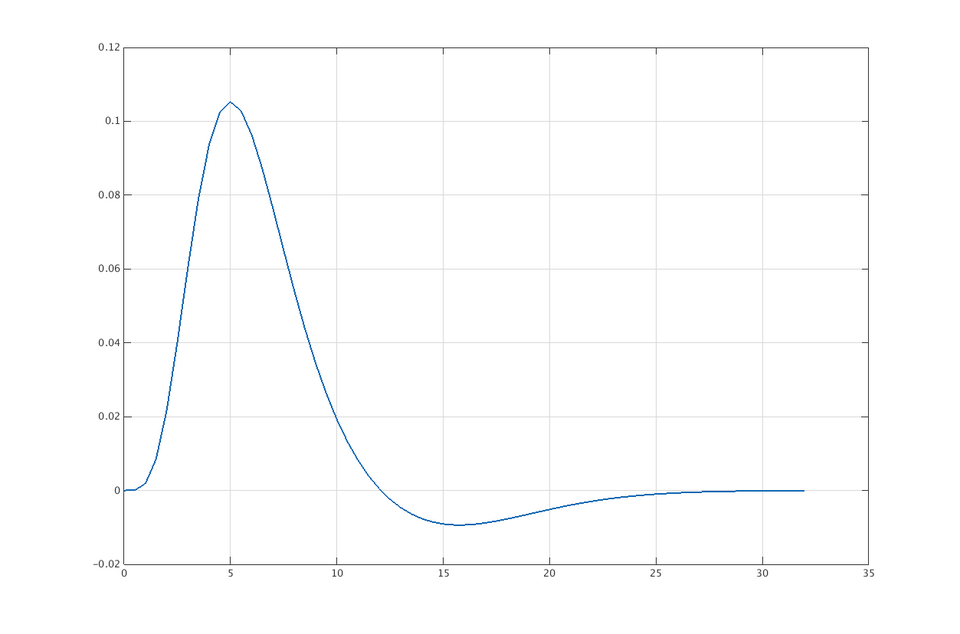
Plot of a canonical hemodynamic response function (HRF), illustrating how the fMRI BOLD signal rises and peaks several seconds after neural activity and then returns toward baseline. This makes the temporal limitation of fMRI intuitive: the measured signal is delayed and temporally blurred relative to neuronal firing. Source
Strengths:
Higher spatial resolution than EEG (better localisation)
Can examine deep brain structures
Limitations:
Lower temporal resolution than EEG (blood flow changes lag behind neural firing)
Typically correlational: activation during a task does not prove the region is necessary for the behaviour
Case studies (in-depth individual evidence)
Case study: an intensive investigation of one individual (or small group), often used when a condition is rare or cannot be ethically induced.
Case studies can reveal how specific brain changes relate to behaviour over time.
Strengths:
Rich, detailed data; can generate hypotheses
Useful for rare injuries or unusual patterns of recovery
Limitations:
Limited generalisability (may not represent most people)
Hard to isolate cause (multiple life factors may contribute)
Lesioning (damage-based inference)
Lesioning: studying the effects of tissue destruction or disruption in the brain (naturally occurring or, in animals, experimentally induced).
Lesion evidence is often used to argue that a brain area is necessary for a function.
Strengths:
Stronger causal inference than purely correlational scans (damage precedes deficit)
Limitations:
Ethical constraints (experimental lesioning is not done in humans)
Real-world lesions are rarely “clean” and may affect networks, not just one spot
Together, plasticity and these methods explain why deficits after injury can improve, why improvements vary across people, and how psychologists connect brain changes to mental processes and behaviour.
Practice Questions
Outline one advantage of using EEG rather than fMRI to study brain activity. (2 marks)
1 mark: identifies EEG has higher temporal resolution / measures rapid changes.
1 mark: links to benefit (e.g., captures quick shifts in activity during a task; fMRI is slower due to blood-flow lag).
Explain brain plasticity and discuss how one brain research method (EEG, fMRI, case study, or lesioning) can be used to investigate changes after brain damage. (6 marks)
1 mark: defines plasticity as reorganisation/rewiring of connections.
1 mark: describes a mechanism or feature (e.g., cortical remapping; synaptic strengthening; greater plasticity earlier in life).
1 mark: links plasticity specifically to recovery after damage (improvement/compensation).
1–3 marks (method use): accurate description of the chosen method plus how it would show change after damage (e.g., fMRI comparing activation patterns pre/post rehab; lesioning linking damaged area to deficit; case study tracking recovery; EEG tracking timing changes).
1 mark (evaluation): one relevant limitation (e.g., fMRI correlational; EEG poor localisation; case study low generalisability; lesions rarely clean/ethical issues).
FAQ
They compare functional outcomes and efficiency over time.
Adaptive: improved performance with streamlined activation.
Maladaptive: persistent pain, inefficient overactivation, or reliance on poor strategies.
Mostly changes in synaptic strength and network connectivity, not brand-new “wires.”
It often involves reweighting existing pathways rather than creating entirely new circuits.
Task design and analysis choices matter.
Differences in baseline performance, rehab intensity, and compensatory strategies can change which regions show heightened BOLD activity.
When the condition is rare or ethically impossible to create experimentally.
Longitudinal case studies can document how behaviour and brain measures shift across months or years.
They use standardised preprocessing and controls.
Remove artefacts (eye blinks/muscle activity)
Use consistent task timing and multiple sessions
Compare against matched control groups

{kind=link}
{kind=link}