
AP Syllabus focus:
‘Disorders such as insomnia, narcolepsy, REM sleep behavior disorder, sleep apnea, and somnambulism can disrupt sleep and affect waking performance and health.’
Sleep disorders reduce sleep quality, fragment normal sleep architecture, and create daytime impairment.
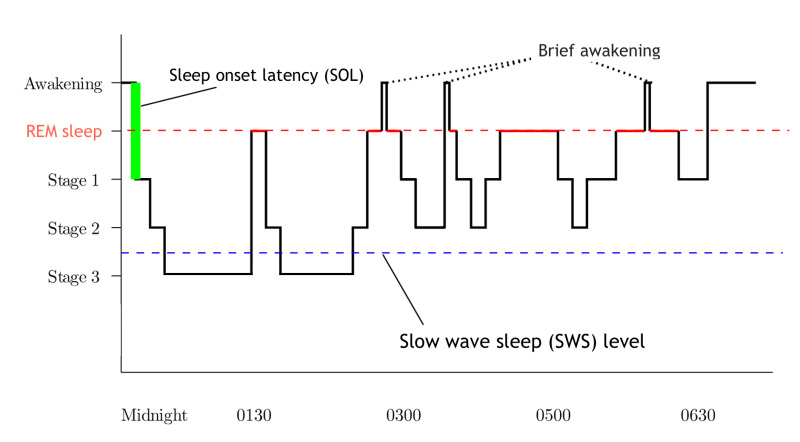
A hypnogram (sleep-stage timeline) showing how an average night cycles through NREM stages (N1–N3) and REM in repeated ~90-minute cycles. It highlights that deep NREM sleep tends to cluster earlier in the night, while REM episodes typically become longer toward morning. This visual makes it easier to see how disorders can “fragment” sleep by increasing awakenings or altering time spent in specific stages. Source
In AP Psychology, focus on how specific disorders disrupt sleep and how that disruption changes attention, mood, learning, safety, and long-term health.
Core idea: disrupted sleep → impaired waking function
Sleep disorders can involve difficulty falling asleep, staying asleep, breathing normally, or staying in an appropriate sleep stage. Common outcomes include excessive daytime sleepiness, reduced vigilance, and increased risk for errors and accidents.
Major disorders named in the syllabus
Insomnia
Insomnia: Persistent difficulty falling asleep, staying asleep, or returning to sleep, accompanied by daytime impairment.
Insomnia often includes fatigue, irritability, and reduced concentration. Because individuals may spend more time in bed without restorative sleep, they can develop anxiety or conditioned arousal around sleep, worsening the cycle.
Narcolepsy
Narcolepsy: A disorder marked by sudden sleep attacks and excessive daytime sleepiness; some cases include cataplexy (sudden loss of muscle tone).
Narcolepsy can intrude into waking life, producing brief but dangerous lapses in alertness (e.g., during driving). Daytime functioning is affected even when total time in bed seems adequate, because sleep-wake regulation is unstable.
Sleep apnea
Sleep apnea: Repeated pauses in breathing during sleep that fragment sleep and reduce oxygenation, often with loud snoring and brief awakenings.
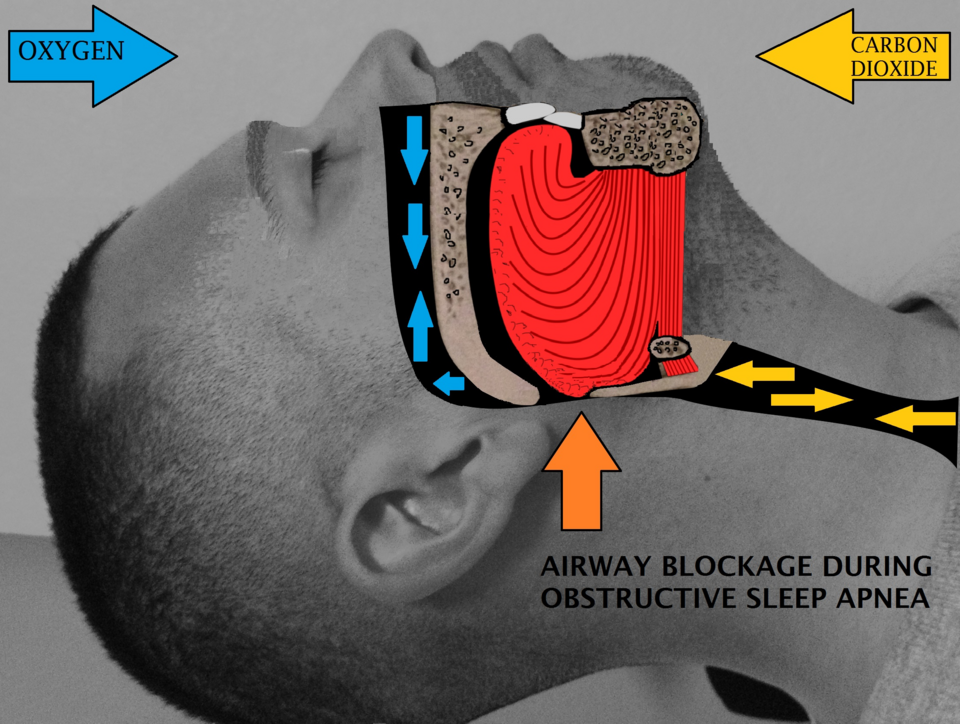
A labeled anatomical illustration of the upper airway during sleep showing how relaxed soft tissue can narrow or block airflow. This directly links the breathing interruption to sleep fragmentation (brief arousals) and reduced oxygenation. It reinforces why sleep apnea often produces pronounced daytime sleepiness and sustained-attention deficits. Source
The repeated micro-awakenings prevent consolidated sleep, leading to pronounced daytime sleepiness and decreased sustained attention. The physiological stress of oxygen drops can also contribute to broader health risks over time.
Parasomnias: REM sleep behavior disorder and somnambulism
REM sleep behavior disorder (RBD) involves acting out dreams due to reduced REM-related muscle paralysis, increasing risk of injury to the sleeper or bed partner. Somnambulism (sleepwalking) typically occurs during deeper NREM sleep, with complex behaviors performed with limited awareness and later poor recall. Both can disrupt household sleep, increase injury risk, and create next-day fatigue due to arousals and fragmented sleep.
Daytime performance effects (what “impairment” looks like)
Sleep disorders commonly disrupt waking performance by affecting:
Attention and vigilance: slower reaction time, lapses in focus, reduced monitoring (higher accident risk)
Learning and memory: weaker encoding and retrieval, more forgetfulness during demanding school/work tasks
Executive functioning: poorer planning, impulse control, and decision-making, especially under stress
Mood and emotion regulation: irritability, lower frustration tolerance, and increased negative affect
Social and occupational functioning: reduced productivity, more conflict, and greater absenteeism
Health consequences linked to chronic disruption
Across disorders, chronic sleep disruption is associated with:
Cardiometabolic strain: elevated stress physiology and increased risk profiles over time (especially emphasized with sleep apnea)
Immune and inflammation changes: greater vulnerability to illness and slower recovery
Safety risks: increased motor-vehicle and workplace accidents due to sleepiness and impaired attention
Quality-of-life decline: fatigue-driven reductions in exercise, motivation, and overall well-being
Practice Questions
State two ways sleep apnoea can affect daytime performance. (2 marks)
Any two from: excessive daytime sleepiness; reduced vigilance/attention; slower reaction time; increased accident risk; poorer concentration at work/school. (1 mark each)
Explain how insomnia and narcolepsy disrupt sleep, and outline two distinct negative effects on waking life or health (at least one effect per disorder). (6 marks)
Insomnia: difficulty initiating/maintaining sleep with non-restorative sleep and daytime impairment. (1)
Narcolepsy: sudden sleep attacks/excessive daytime sleepiness (credit cataplexy if described). (1)
Effect linked to insomnia (e.g., impaired concentration, mood irritability, reduced executive functioning, fatigue). (2 max; 1 per well-described effect)
Effect linked to narcolepsy (e.g., dangerous sleep attacks affecting driving/safety, learning disruption from sleepiness). (2 max; 1 per well-described effect)
FAQ
Common approaches include:
CPAP (continuous positive airway pressure) to keep the airway open
Oral appliances to reposition the jaw
Weight management or positional strategies in some cases
Reducing breathing pauses decreases micro-awakenings and oxygen drops, which typically improves vigilance and daytime energy.
Polysomnography can rule out other causes (e.g., sleep apnoea).
A Multiple Sleep Latency Test (MSLT) assesses how quickly a person falls asleep across scheduled daytime naps and whether REM sleep appears unusually fast, supporting narcolepsy diagnosis.
In some individuals, RBD is associated with later development of neurodegenerative conditions involving brain systems that regulate movement and REM muscle atonia.
It is not deterministic, but it can prompt monitoring and early clinical attention.
Risk reduction can include:
Securing windows/doors and removing sharp objects
Using alarms or motion sensors
Avoiding sleep deprivation and alcohol, which can increase episodes
If episodes are frequent or dangerous, professional evaluation is recommended.
CBT-I (cognitive behavioural therapy for insomnia) targets maintaining factors such as conditioned arousal, unhelpful sleep beliefs, and inconsistent schedules.
Medication can help short-term for some people, but behavioural approaches aim for durable change without tolerance or rebound sleep problems.

{kind=link}